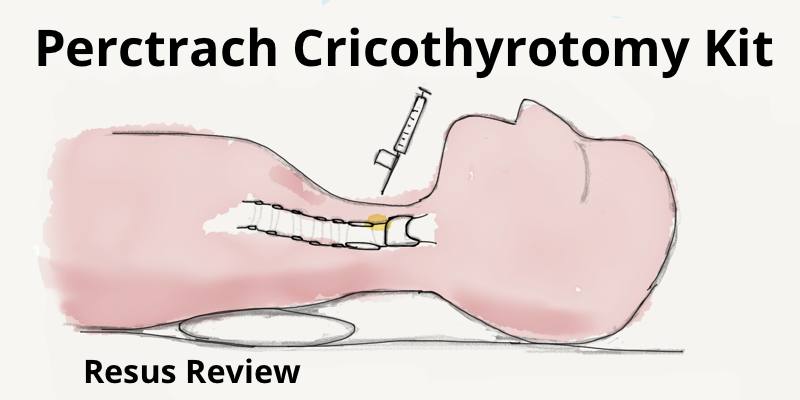
Pertrach Emergency Cricothyrotomy Kit
Pertrach Emergency Cricothyrotomy Kit uses an innovative finding splitting needle to enter the cricothyroid membrane, and allows the dilator to be inserted without requiring a Seldinger wire.
Pertrach Emergency Cricothyrotomy Kit uses an innovative finding splitting needle to enter the cricothyroid membrane, and allows the dilator to be inserted without requiring a Seldinger wire.
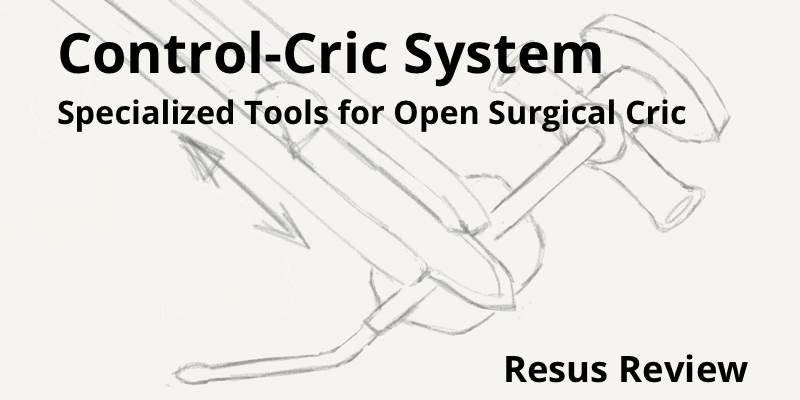
The Control-Cric System has been developed by Dr Richard Levitan to allow for increased success and speed of performing an emergent cricothyrotomy. It includes a specially designed scalpel (Control-Knife) and custom tracheostomy tube (Control-Key).
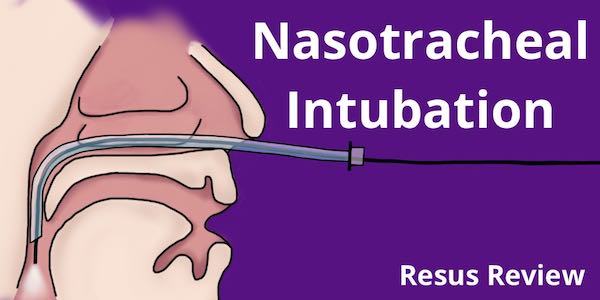
Nasotracheal intubations are useful technique in a number of situations including distorted airway anatomy and awake intubations. Patient preparation and anesthesia are key. Understand how to use the endoscopes and the procedural steps for a successful and safe nasotracheal intubation.

Intubating and non-intubating supraglottic airways (LMA) for neonates and children are an important tool for managing the emergency pediatric airway. Depending on the product, they have unique features that can help facilitate BVM ventilation, provide gastric suctioning, or allow for intubation directly or over a bronchoscope. Learn how to use the air-Q LMA, LMA Supreme, LMA Fastrach and how they can be incorporated as a critical part of your pediatric airway algorithm.
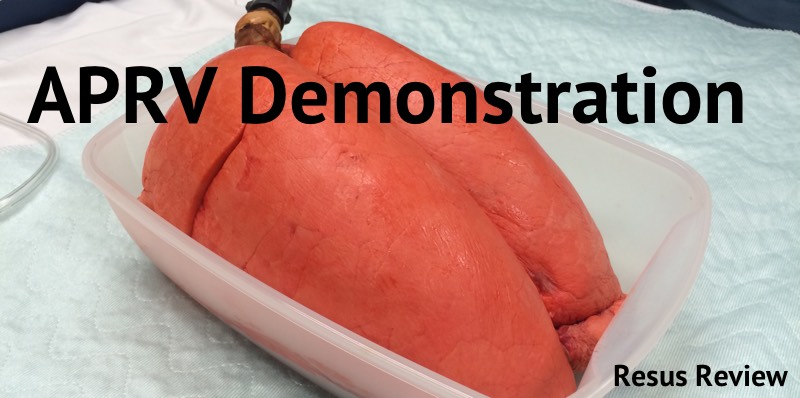
Demonstration of mechanical ventilation using APRV to understand how the lungs behave.
During a percutaneous tracheostomy procedure, the edge of the Shiley tracheostomy tube can catch on the tracheal rings deforming the shape and making it difficult to cannulate into the trachea. This can occur even if the bevels of the Shiley and trocar are aligned perfectly.
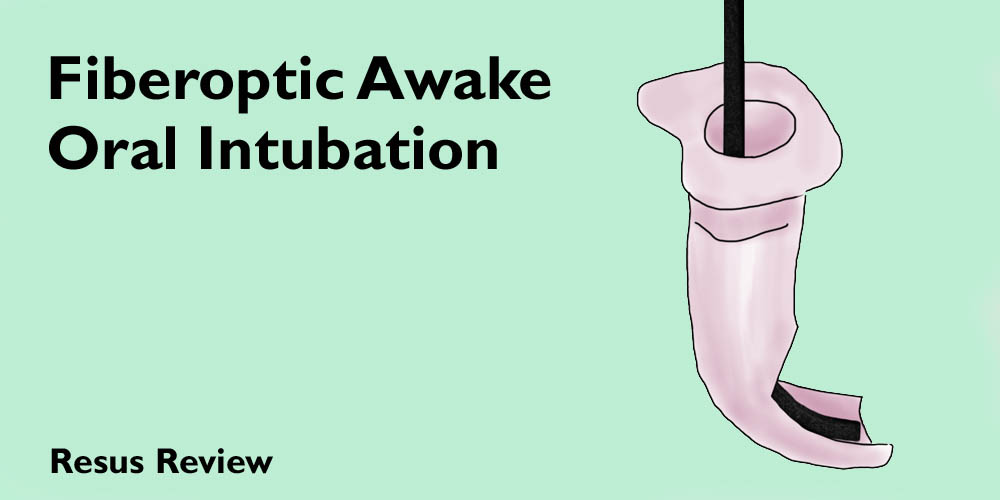
Fiberoptic oral intubation with flexible fiberoptic scope is useful technique for intubating a patient in respiratory distress which it is desirable to maintain spontaneously breathing during the intubation. Tutorial and procedure steps for performing fiberoptic awake oral intubation including equipment, preparation, and medications.
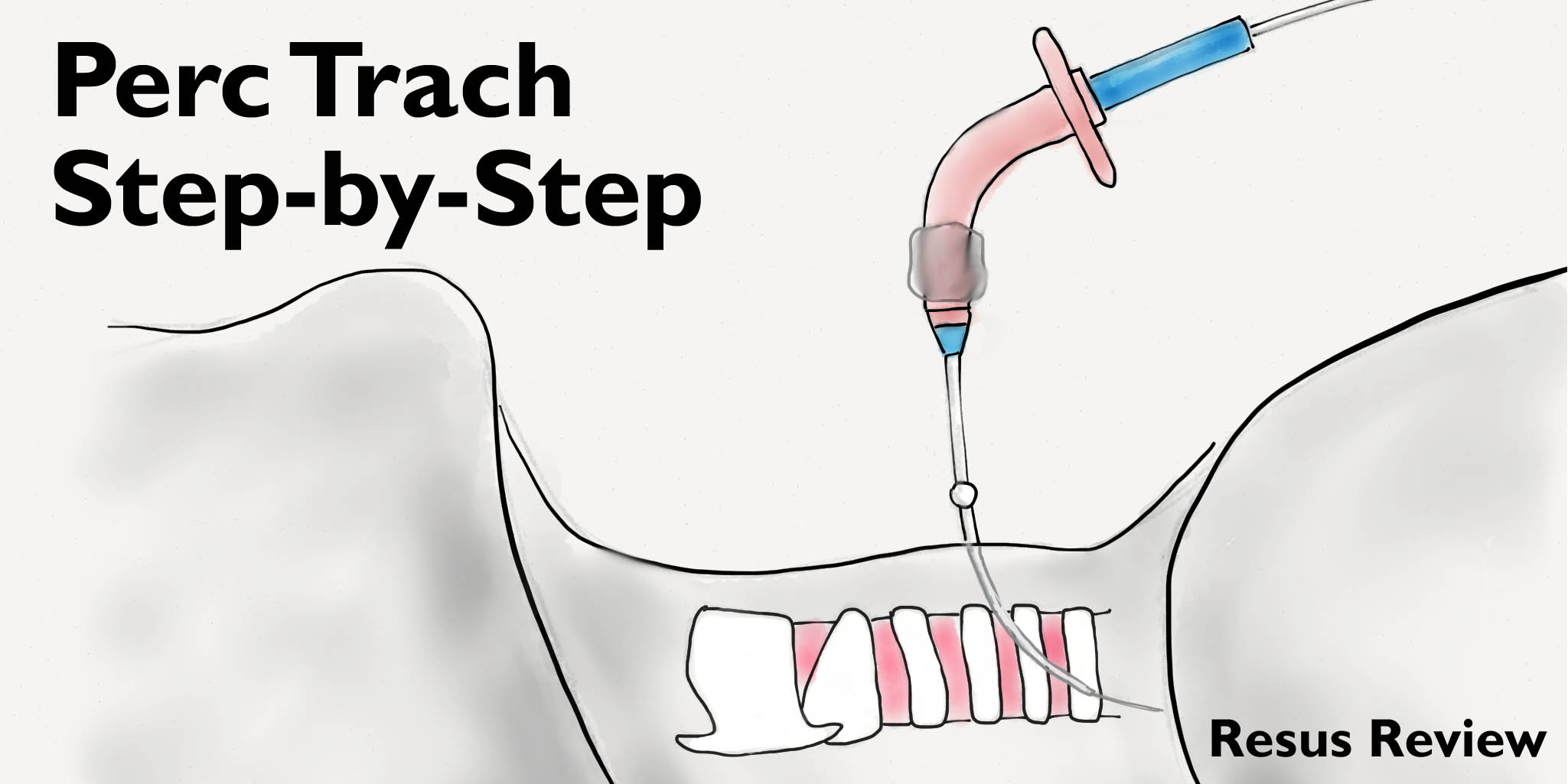
For patients that require prolonged mechanical ventilation, a tracheostomy can be placed either in the operating room as an open surgery, or more preferably at the bedside with a minimally invasive procedure in the intensive care unit by a percutaneous dilational technique under bronchoscopic guidance. This is a step-by-step tutorial for patient selection and procedure techniques.

A frustrating type of difficult intubation occurs when you are able to cannulate the trachea, but are unable to pass the endotracheal tube. This case is of a patient who had a decannulated tracheostomy and developed subglottic tracheal stenosis.

Case of a cardiac arrest patient who was intubated in the field with a King Supraglottic Airway. He arrived in the ED with on going BVM ventilation. A cervical spine x-ray showed the distal tip of the King Airway had accidentally folded in the pharynx.
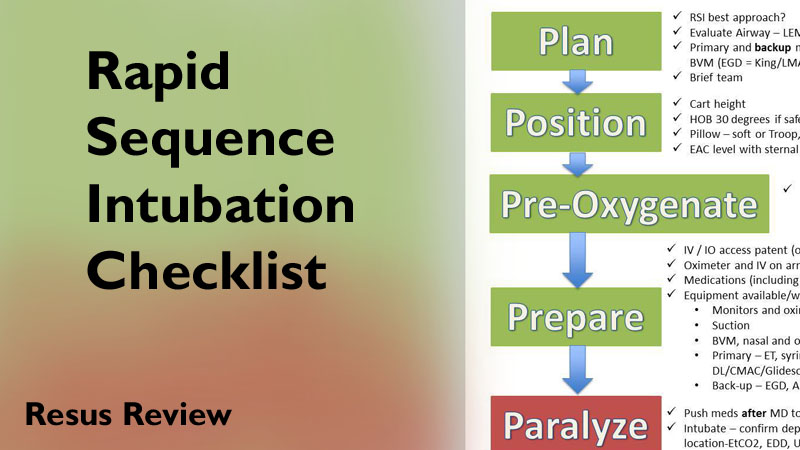
HCMC has created a rapid sequence intubation (RSI) checklist, and printed it in large poster format. It is hung above our airway cart in the stabilization bay. This is organized around the 'P's. There are more detailed considerations under each heading to the right as well. This checklist is designed to be a quick visual reference during RSI to remind you to plan, position, pre-oxygenate (and provide apneic oxygenation with nasal cannula), and be deliberate with your preparation and decision-making. Most importantly, it includes post-intubation steps, that can often be overlooked as the team moves on to other resuscitation steps after securing the airway.
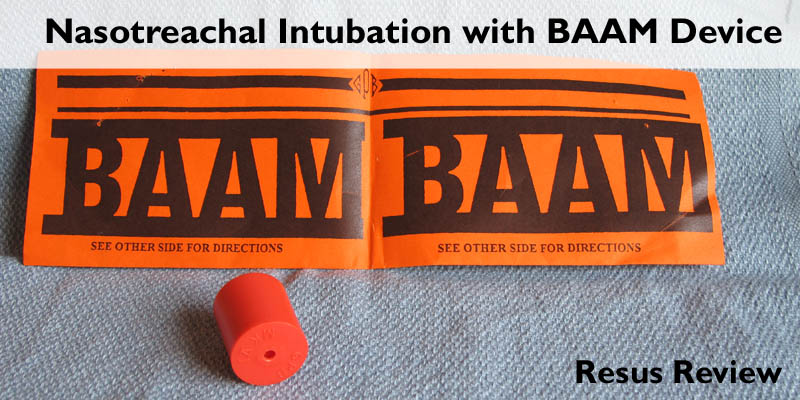
Nasotracheal intubation is an essential skill that allows a flexible approach to airway management. The BAAM device can speed and simplify both your blind and fiberoptic nasotracheal intubations. Instructions on proper use including patient selection.