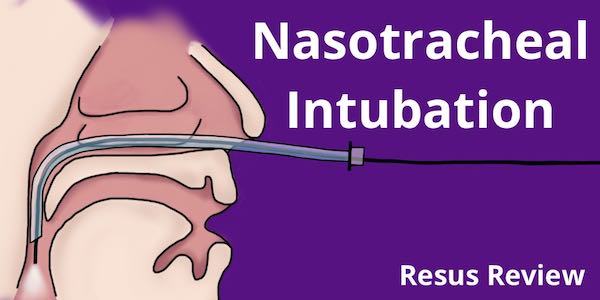
Nasotracheal intubation is an essential skill that allows a flexible approach to airway management. These are generally performed with the patient awake and spontaneously breathing and protecting their airway. They can either be performed with a endoscope or blindly.
In order for blind nasotracheal intubation to be successful it requires patient respiratory effort and air exchange so that you can listen for air movement from the end f the endotracheal tube. The Beck Airway Airflow Monitor (BAAM) is a device which when attached to a 15 mm endotracheal tube adapter, magnifies airway-airflow sounds, producing a whistling sound which greatly aids in correct endotracheal tube placement.
 |
 |
Below you can see it attached to the 15mm adaptor of an endotracheal tube.

There are two camps in Fiberoptic Bronchoscope-assisted nasotracheal intubation: Tube-before-Scope and Scope-before-Tube (Roberts and Hedges has a discussion for advantages of each). The BAAM device is only used in the Tube-before-Scope approach. BAAM can be helpful with Fiberoptic Bronchoscope NTI if it is your practice to place the ETT into the hypopharynx before inserting the tube. Ideally, it gets you close enough to the inlet so that, when you place the scope and it peeks out the tube end, the cords are sitting in front of you (The device has a small hole in the end which creates the whistle when the pt breaths- it is not for an scope). BAAM is not used if the bronchoscope is placed before the ETT.
The impetus for getting the BAAM has been several cases of severe angioedema that have had prolonged intubation times. The BAAM may also help position the ETT for a blind pass which. Even if you’re not expert in BNTI, you have nothing to lose: if the ETT is in good position, the pt is in sniffing position, and you attempt tube passage just as pt initiates a breath, you are often successful.
Location of the BAAM device on the airway cart.
Instructions
- Attach the orange BAAM device to the 15 mm adaptor of the appropriate sized endotracheal tube, the device will attach only one-way to the tube.
- Pre-oxygenate and/or ventilate while preparing the patient for nasotracheal intubation.
- Perform nasotracheal intubation. As the ET Tube nears the larynx an audible increase in whistling will be heard from the device, indicating that the tip of the endotracheal tube is near the entrance to the trachea.
- Carefully advance the endotracheal tube through larynx into the trachea when device and airway sounds are at their peak. Confirm that successful intubation has occurred.
- Once intubated, quickly remove the BAAM device and begin ventilating the patient.
- Confirm tube placement by visualization, auscultation, and/or capnography.
Precautions
- An unobstructed endotracheal tube with its tip located in the pharynx can also produce the whistle sound, therefore, it is important to always confirm placement in the trachea.
- Due to the narrow aperture of the BAAM device, it is never to be left attached to the endotracheal tube for greater the 15 seconds at any time for assessment of the previously intubated patient. Partial airway obstruction, hypoxia and increased airway pressure can occur if left in place for prolonged periods of time.
Indications
- As an adjunct to blind nasotracheal intubation in the patient with spontaneous respirations.
- As aid to re-confirming airway patency or re-assessing respiratory effort in the intubated patient with respiratory effort. This device is not to be used as the primary method for assessing airway patency in the intubated patient.
Contraindications
- Apnea or inability to hear device during endotracheal tube insertion.
References
- Cook RT Jr, Stene JK Jr.. The BAAM and endotrol endotracheal tube for blind oral intubation. Clin Anesth. 1993 Sep-Oct;5(5):431.

If the BAAM whistle is not available, one can pull off the auscultation head of most stethoscopes and insert the tubing (if not oversized) into the ETT lumen and use it to find the loudest airflow and thereby align with the glottic opening; pass tube upon inspiration when the cords are apart.
Great tip. Thanks for sharing.