Nasotracheal intubation is an invaluable tool for securing a definitive in patients where laryngoscopy (either direct or video) would be difficult or has failed. This technique is especially helpful when intubating the patient awake. Endoscope intubations can also be performed orally or even blindly, which we have covered before. Nasotracheal route is generally preferred over the oral route in awake patients because it is better tolerated and the path to supraglottic space is more direct from the nasopharynx. Situations to consider nasotracheal intubation include:
- Distorted upper airway anatomy from angioedema, hematoma, or abscess (think Ludwig angina)
- Maintaining patient’s respiratory drive
- Cervical immobilization
- Upper airway burns
- Can’t intubate, CAN oxygenate failed airways (must be able to bag)
Nasotracheal intubation is generally well tolerated. Visualization can be difficult with excessive secretions or blood in the airway.
Intubating Endoscopes
There are many different types of endoscopes available. The traditional bronchoscope (600mm length) can be used, but often is not readily available in the emergency department and comes on a cart or tower that is cumbersome to use. A portable handheld bronchoscope with an eyepiece and self contained light-source (such as made by Machida Corporation) are handy, but again rare to find outside of intensive care units and endoscopy suites. Development of non-fiberoptic endoscopes that have an integrated camera and light sources at the tip of the scope have been developed and are called flexible video intubating endoscopes (available from both Olympus and Storz). The attach to small portable video monitors that can be positioned bedside. These scopes tend to be shorter in length (400mm as compared to 600mm), and a smaller tip diameter of 3mm. The working channel for suction also tends to be a small diameter.
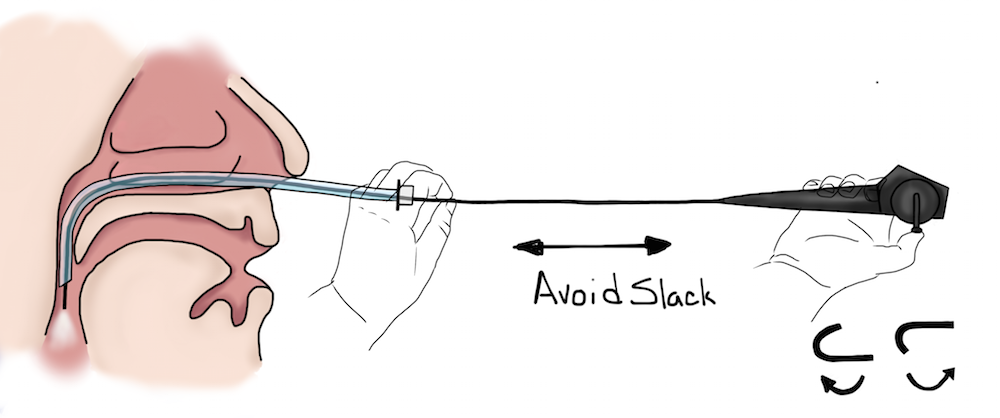
Endoscopes can move in 3-degrees of freedom. In and out is the axial motion along the length of the scope. Rotating the scope provides rotational control. Avoid slack or U-shapes in the scope. When this occurs, any rotation of the scope head will not be translated to the scope tip and you will lose rotational control. The tip of the scope can be flexed up or down with the thumb control.
Supplies for Nasotracheal Intubation
- Endoscope
- 2% lidocaine viscous
- 4% lidocaine cream (LMX4)
- 4% lidocaine liquid
- Endotracheal tube (generally 5.5-6.5 size)
- Lubricant
- Phenylephrine or oxymetazoline
- Cetacaine spray (optional)
- Sedation medications (see below)
Patient Preparation and Anesthesia for Nasotracheal Intubation
The key to performing awake nasotracheal intubations is patient preparation and achieving adequate anesthesia of the intubation path.
- The patient can be positioned in a lying or sitting position. For awake patients, a more upright position is preferred. The intubator can either be at the patient’s head (traditional intubating position), or at the patient’s side facing the patient. If patient is sitting, place a pillow or towels behind the patient’s head to prevent extension while intubating.
- Occlude one nare at a time to verify that the patient can breath through each one. Choose the larger one.
- Treatment of the nasal passage with aerosolized phenylephrine or oxymetazoline can help reduce mucosal trauma.
- Instill lidocaine 2% viscous gel into the nare you intend to use for the endoscope. Use a cotton tipped swab or your finger to ensure that the lidocaine is coating the entire surface and to dilate the nare. Have the patient sniff it back, and run down the back of their throat.
- Apply a large dolop of lidocaine 4% cream (LMX4) to a tongue blade. Using a 4×4 apply gentle traction to the patient’s tongue to pull it forward and apply the lidocaine to the back of the patient’s tongue. Have them gargle the cream as it runs down the back of their throat
- If time allows, give glycopyrrolate to control secretions. If is effective, but can take up to 20 minutes for complete drying.
- Topical cetacaine spray can be used, but adequate preparation with the lidocaine often provides enough anesthesia.
- Preoxygenate as usual.
Topical anesthesia is key, but do be very careful for lidocaine toxicity especially in smaller patients. Lidocaine is very well absorbed through mucosal tissues, so consider any that you give or apply as completely absorbed. Lidocaine 4% is 40mg/cc. In small a smaller person with bad gag reflex, there have been instances of lidocaine toxicity and death. Toxicity develops at 4.5mg/kg max (rounded down to 4mg/kg for calculation simplicity). A 50kg person (110lbs) would max at about 200mg or 5cc of 4% lidocaine
Nebulized lidocaine does not usually provide enough anesthesia because most of the medication goes into the alveolar space. An atomizer, is useful though because it makes larger drops that condense in the naso and oropharynx. An LTA works good for this.
Sedation for Awake Intubations
There are many options for sedation during awake nasotracheal intubation. The perfect agent would provide enough sedation and anesthesia, while allowing the patient to continue spontaneous respirations and airway protection. Often, with enough topical anesthesia preparation patient’s do not require large amounts of sedation. The dissociative anesthetic ketamine works very well.
Recent studies support the use of the clonidine analogue centrally acting alpha2 medication dexmedetomidine, and it may better tolerated than propofol, remifentanil, sufentanil, or etomidate for awake NTI. Use it at 1.0 mcg/kg IV over 10 minutes and then 0.5 mcg/kg/hr infusion. A recent study in J Craniomaxillo Surg compared dexmedetomidine alone to dexmedetomidine + ketamine, and there were less hemodynamic complications (bradycardia) from the dexmedetomidine, so that would be reasonable approach.
Atypical antipsychotics olanzapine, droperidol, and even ziprasidone are commonly used. The very short acting opioids — remifentanil, sufentanil, and alfentanil have been reported in the literature. Carefully titrated propofol, etomidate, or benzodiazepines (midazolam, ativan, etc) are also reasonable alternatives, though the possibility of inducing deep sedation is greater.
Nasotracheal Intubation Procedure Steps
- Make sure patient is thoroughly prepared, anesthetized, and preoxygenated.
- Verify with your team the intubation steps and that all equipment is available.
- Lubricate the endotracheal tube and load it on the bronchoscope.
- Provide sedation as needed (see above).
- Enter the nare and advance along the floor of the nasal cavity (ie go straight backwards, do not follow the contour of the bridge of the nose).
- Navigate the endoscope around the bend of the posterior nasopharynx, and advance to the hypopharynx where you should be able to visualize the vocal cords.
- Once the endoscope is in position, advance the ETT to the level of the uvula (preloading the ETT in the nasopharynx).
- Through the port, inject 1-2mL of lidocaine 4% liquid directly onto the vocal cords and laryngeal inlet.
- The endoscope should be advanced slowly to just above the cords, and during a patient’s inspiration cannulate the endoscope through the cords.
- Verify you are in the trachea by directly visualizing the membranous trachea, cartilaginous trachea, and carina.
- Additional lidocaine 4% liquid can be instilled in the trachea and at the carina to minimize cough.
- Advance the endotracheal tube through the cords.
- The correct depth positioning of the ETT can be achieved by using the endoscope to measure the distance between the carina the ETT inlet. A distance of approximately 4cm is usually adequate for adults.
- Fully sedate the patient. Paralytics are not usually necessary at this point.
- Secure the ETT and
- Functional verification of placement with US or EtCO2 capnography is reasonable. Verification of depth with a chest radiograph is not needed if you have physically measured the depth with the endoscope.
Contribute your thoughts.