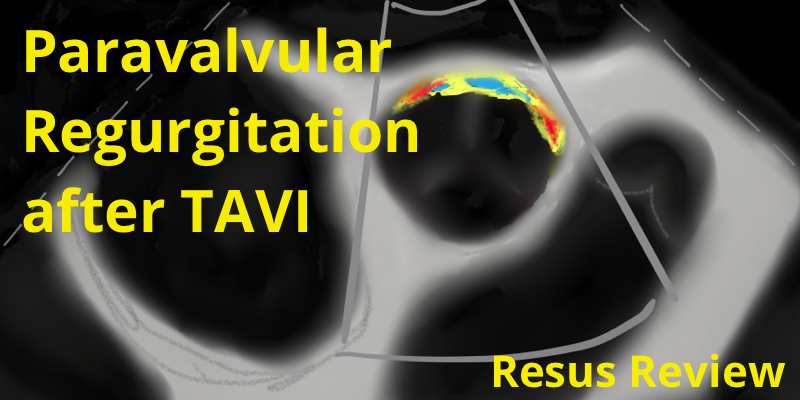
Paravalvular regurgitation after transcatheter aortic valve implantation occurs in in over 50% of patients, and correlates with 1-year mortality. The regurgitant jets are best characterized with transesophageal echocardiography to define the circumferential extent and cross-sectional area. Overtime, most the regurgitation decreases, and occasionally disappears completely.
Transcatheter cardiac interventions are a fast evolving field. The past decade has seen the development of transcatheter aortic valve replacement, transcatheter mitral valve repair and replacement, septal defect closure devices and left atrial appendage closure devices for thromboprophylaxis.
Left main stem disease is associated with significant morbidity and mortality. Coronary artery bypass surgery has been the definitive treatment choice. However, advancements in percutaneous coronary intervention (such as drug-eluting stents and techniques, risk stratification, and intravascular ultrasound) have increased the viability of this treatment option.
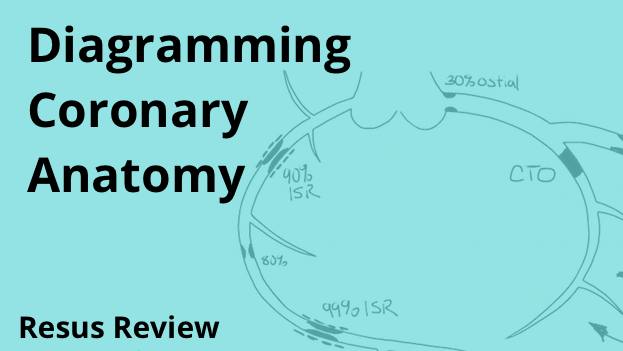
Coronary arteries can be difficult to visualize, especially when there are multiple lesions, interventions, and grafting. Diagramming the anatomy allows you to track lesions, stenting, grafts, size size/variation of native arteries. It is a useful technique for your own understanding and facilitating communication.
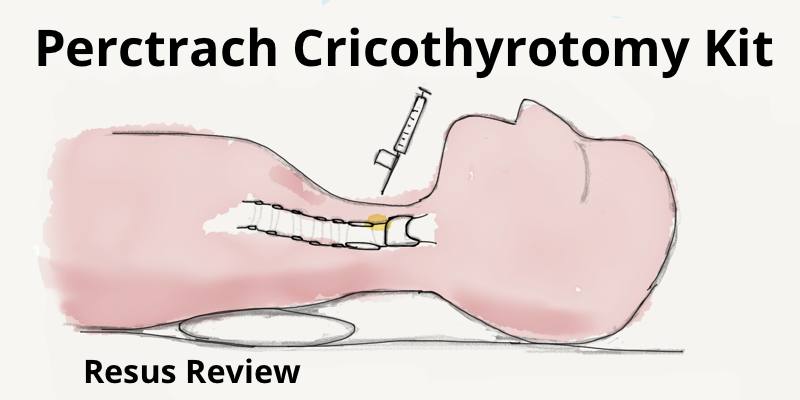
Pertrach Emergency Cricothyrotomy Kit uses an innovative finding splitting needle to enter the cricothyroid membrane, and allows the dilator to be inserted without requiring a Seldinger wire.
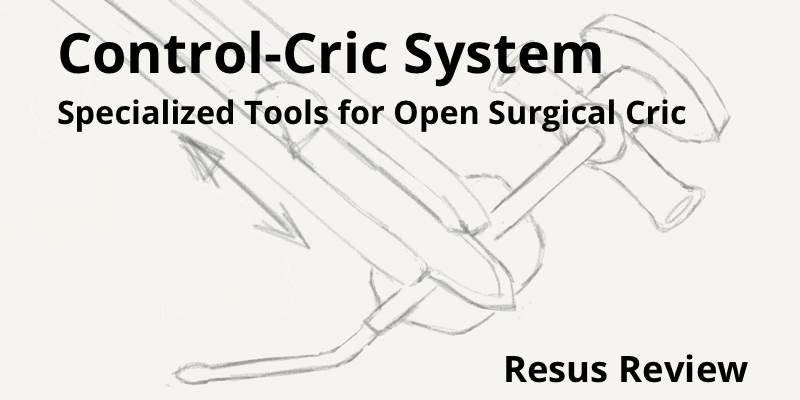
The Control-Cric System has been developed by Dr Richard Levitan to allow for increased success and speed of performing an emergent cricothyrotomy. It includes a specially designed scalpel (Control-Knife) and custom tracheostomy tube (Control-Key).
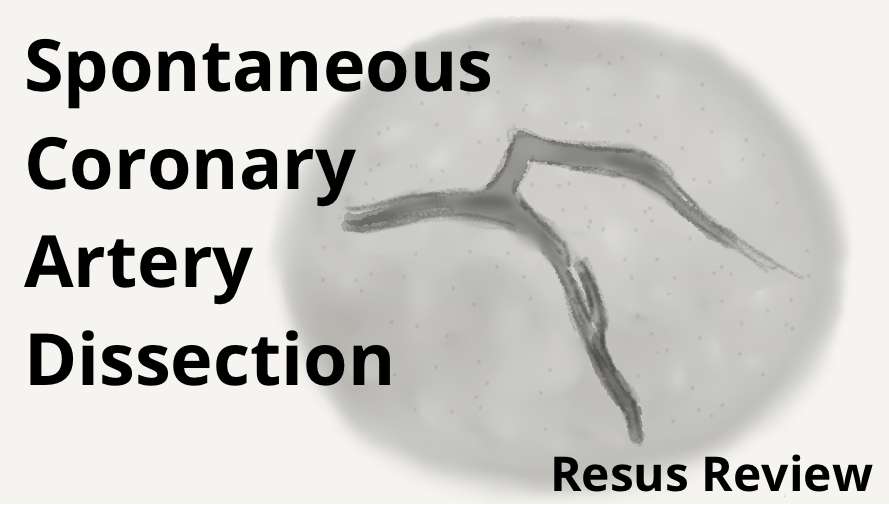
Spontaneous coronary artery dissection (SCAD) is a non-traumatic and non-iatrogenic separation of the coronary artery wall that is now recognised as an important cause of myocardial infarction, especially in younger women or those without traditional cardiovascular risk factors.
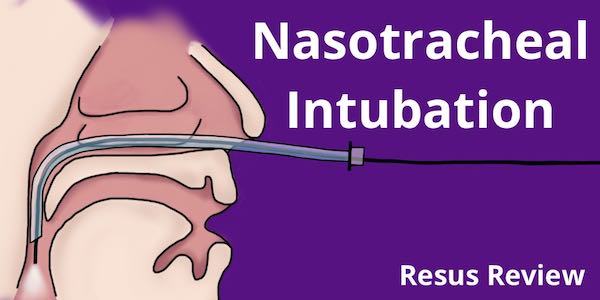
Nasotracheal intubations are useful technique in a number of situations including distorted airway anatomy and awake intubations. Patient preparation and anesthesia are key. Understand how to use the endoscopes and the procedural steps for a successful and safe nasotracheal intubation.
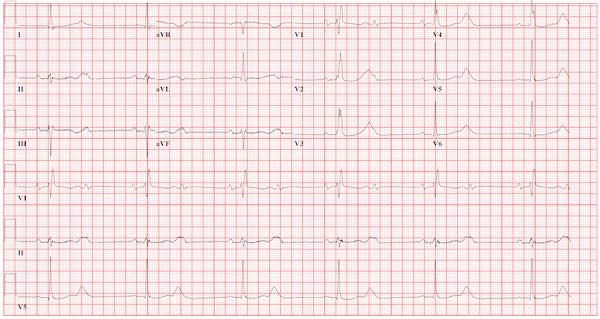
Symptomatic bradycardia and high degree AV block puts patients at high-risk for decompensation. While ischemia is a concern with all new conduction abnormalities. However it is a common development in patients with recent aortic valve replacement and often requires permanent pacemaker.
Detailed ECMO safety checklist to be performed at every shift change for nurses, perfusionists, and physicians. Includes data review and bedside equipment inspection.

Intubating and non-intubating supraglottic airways (LMA) for neonates and children are an important tool for managing the emergency pediatric airway. Depending on the product, they have unique features that can help facilitate BVM ventilation, provide gastric suctioning, or allow for intubation directly or over a bronchoscope. Learn how to use the air-Q LMA, LMA Supreme, LMA Fastrach and how they can be incorporated as a critical part of your pediatric airway algorithm.
Understand the workings and tips for best use of ECMO ultrasonic sensors. ECMO centrifugal flow pumps require external sensors to provide accurate measurement of blood flow rates based on differential acoustic transit time due to the Doppler effect. The acoustic mirror of bubbles allow for easy detection of air in the line also.