One of the major risks of right heart catheterization in the ICU is pulmonary artery rupture. While exceedingly rare (0.06% – 0.2%), it has a high mortality of approximately 50% usually within 30 minutes. When I was first learning about pulmonary artery catheters, I envisioned this primarily as a problem with the distal tip of the catheter migrating into the small vessel and capillary bed, which then is rupture during balloon inflation. I felt secure that this serious complication was eliminated by ensuring proper tip positioning. Unfortunately, like everything in medicine the reality is more complicated.
Mechanisms of rupture
- Balloon over distension of small artery, arteriole or capillary.
- Local trauma to the vessel wall by the pulmonary artery catheter tip.
- Eccentric wedging of the balloon.
Risk Factors
- Mechanical factors (rapid balloon inflation, distal catheter position, rigid catheters)
- Poor compliance of pulmonary arteries (pulmonary hypertension, older patients)
- Heparinization
During patient repositioning, transport or patient movement, the pulmonary artery catheter may migrate distally and become wedged. This spontaneous wedge happens without balloon inflation and may cause pulmonary infarction, but not necessarily pulmonary artery rupture. It can be detected by a change of the pulmonary artery waveform to a wedged waveform. This is the reason it is critical to monitor pulmonary artery pressure continuously.
In our patient, a brief episode of arrhythmia was noted as the catheter was floated through the right ventricle (see below). The pulmonary artery catheter should be moved through the right ventricle rather quickly. If the catheter requires re-positioned, the balloon should be deflated and the catheter withdrawn completely to the right atrium before attempting the repositioning to minimize time in the right ventricle.

We were able to correctly flow the pulmnonary artery catheter and obtain a normal appearing wedge waveform. Good practice is to inflate the balloon slowly while observing the pressure tracing on the monitor. When the pressure changes from PA to Wedge no more air should be inserted. TAfter wedging the catheter always make sure the monitor returns to a PA trace.

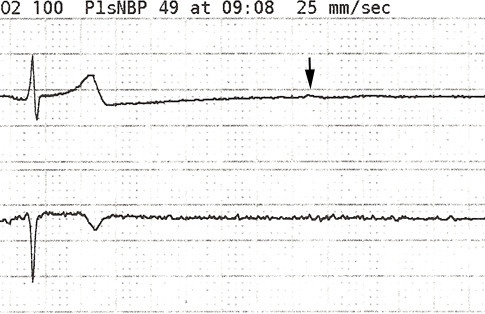
Several hours later, however, when the wedge pressure was measured the following tracing was obtained at 1mL balloon inflation.

The upward curve of the pressure tracing was immediately noticed, the the physician immediately deflated the balloon. That increasing pressure is a serious risk of pulmonary artery rupture. The position of the catheter tip was verified to be correct in the right main pulmonary artery.
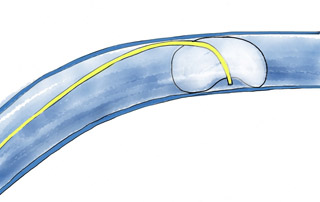
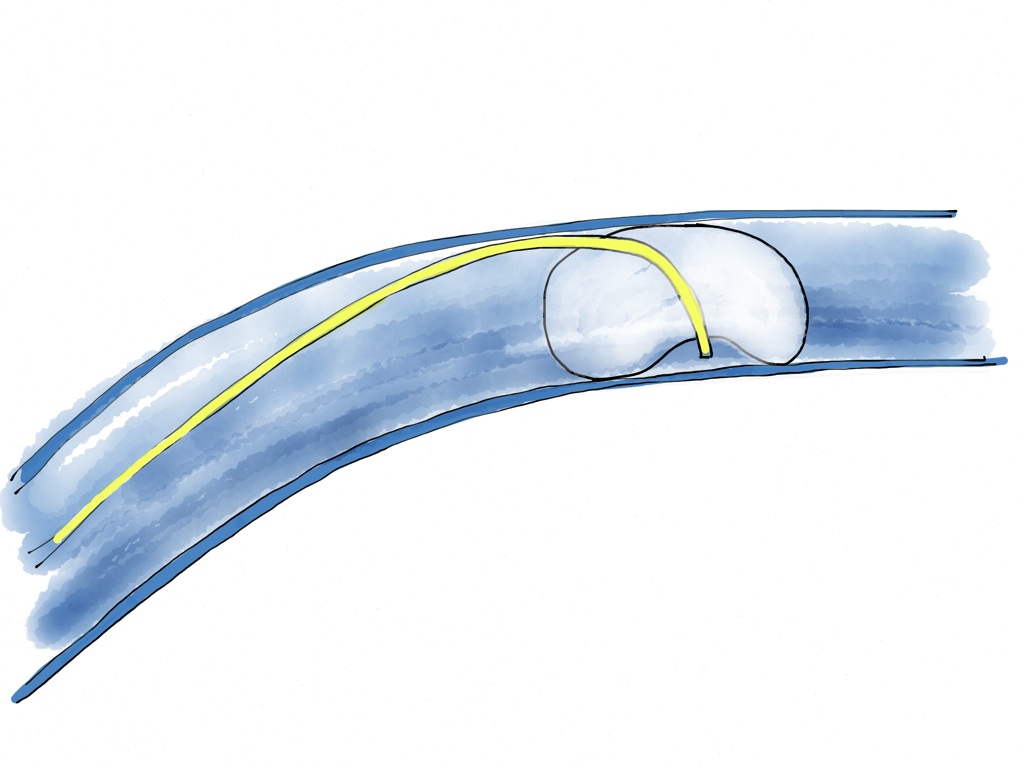
The most common cause of overwedging when the catheter tip is correctly positioned is an eccentric wedge (see figure below). The balloon traps the catheter tip against the vessel wall.Since there is a constant fluid flow through the distal tip to prevent clot formation, the fluid builds up an increases the pressure in the trapped cavity which places the vessel at risk for rupture.
If there is not an actual defect in the balloon causing it to be eccentric (you did verify its inflation before insertion correct?), the problem of eccentric wedging can usually be corrected by repositioning the catheter tip by slightly (~1cm).


Contribute your thoughts.