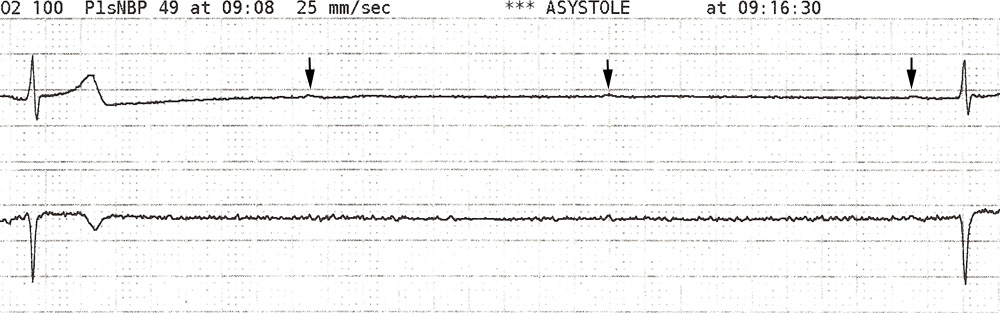
Unfortunately procedural complications can occur on the backside of procedures as well as during the intervention phase of the procedure. Look at the rhythm strip shown below. This is a 50-year-old man who had developed septic shock from Streptococcus pneumonia. He had done quite well though. His hemodynamics had normalized and he was no longer requiring inovasopressor support. He had been extubated the day before without any signs of respiratory distress. He was weak from his 10-day ICU stay, but was ready to be transferred to the general medicine ward.

This was puzzling. The patient was getting better. Why would he be developing arrhythmias at this point in his hospital course. As I investigated the issue it turned out that the nurse was removing his central line when this occurred. Ahhhh..now that made sense. Vagal stimulation from the removal of the CVC and carotid massage from holding pressure to achieve hemostasis had lead to excessive vagal tone which caused AV nodal blockade.
Interestingly you can also see the impact of vagal tone the SA node. An enlarged view of the transient asystole period shows p waves, though at a bradycardic rate that is about 30% longer than the baseline rate.
The patient continued to do well, and had no further arrhythmia events. He made a complete recovery from his septic shock and pneumonia.

Contribute your thoughts.