The JAMA series on Rational Clinical Examination has taught us that each physical exam maneuver needs to be evaluated with an evidenced-based assessment, that includes sensitivity and specificity. We have learned through the series that many specific exams are near worthless, while others provide some value though far less than we may have been led to believe during our medical school and residency training.
![]()
The knowledge of the fall failings of the traditional physical exam, and the near universal availability of bedside ultrasound has changed the physical exam fundamentally and forever. Many previous exam maneuvers such as palpating ventricular heave or PMI, are distant markers of what you fundamentally care about which is cardiac function. With ultrasound that gives you direct visualization of structures, ventricular function can be directly interpreted even by novice registrars.
A stethoscope, reflex hammer, or pen light are tools that aid my physical exam. Ultrasound is just another tool, that quickly an easily lets me answer questions during my physical. There is nothing that feeling for abdominal bruits can tell me that cannot be more quickly and more definitively answered with an abdominal probe in your hand.
In the United States, Medicare billing requires a certain number of physical exam bullets fore a specific level of billing which prompts physicians to continue performing useless physical exam maneuvers on patients, or even worse document that they performed them without actually doing so. While unethical, this grows out of a frustration with documentation requirements that do not fit with our current knowledge and practice of medicine. it is also unethical for Medicare to subject the patient to fruitless parts of the physical without any benefit to their care.
The other billing issue is the requirements for billing for the ultrasound. Per CMS, the following three components are necessary.
- Interpretation – a written interpretation and report must be completed and be maintained in the patient’s medical record. The report must describe the structures or organs studied and supply an interpretation of the findings.
- Medical necessity – the medical record documentation must indicate why the test was medically necessary.
- Image Retention – appropriate image(s) with measurements when clinically indicated of the relevant anatomy / pathology must be permanently stored and available for future review. Please note that an image is now required for all procedures performed with an ultrasound.
It is my opinion, these requirements are met with this new format.
What I have become a strong advocate for, is incorporating my ultrasound findings directly into my physical exam documentation. Assessments made by ultrasound should be viewed as tests answering questions, and should documented accordingly.
Below I shown an example comprehensive physical exam of a patient presenting with shortness of breath, who has decompensated heart failure. I have highlighted the items included based on ultrasound.
PHYSICAL EXAMINATION
Vital Signs: BP 128/68 | Pulse 111 | Temp 37.7 °C (Oral) | Resp 24 | Wt 118.8 kg | SpO2 89% on room air.
Constitutional: Mild respiratory distress. Does not appear toxic.
Eyes: White and quiet. PERRL (R 3~2 | 3~2 L).
ENMT: Moist oral mucosa. No tonsillar exudates or hypertrophy. No swelling or erythema of posterior oropharynx.
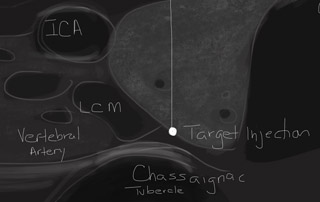
Neck:
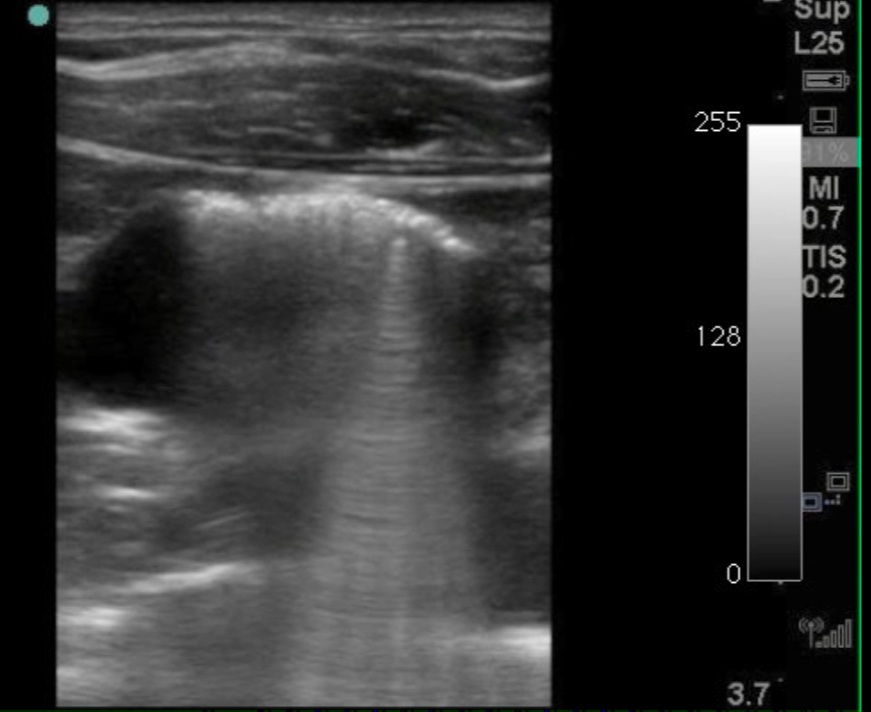
Respiratory: Increased effort. Rales bilaterally. Sliding lung signs present bilaterally. Approximately 12 B-lines bilaterally. No significant pleural effusion.
Cardiovascular: Regular tachycardic rhythm. Soft S3 heard with no murmur. No pericardial effusion. Dilated cardiac structure. Moderately decreased cardiac function. Proximal thoracic aorta 20mm. No significant aortic valve or mitral valve stenosis. E-point septal separation is 12mm.
Gastrointestinal: Soft. No tenderness to palpation. No intraperitoneal free fluid. Maximum abdominal aorta diameter 2.9 cm. IVC diameter 2.4cm with no respiratory variation. Bladder decompressed with Foley catheter balloon in place.
Genitourinary: Foley catheter in place.
Neurologic: No deficits of cranial nerves. Strength and sensation normal in bilateral upper and lower extremities.
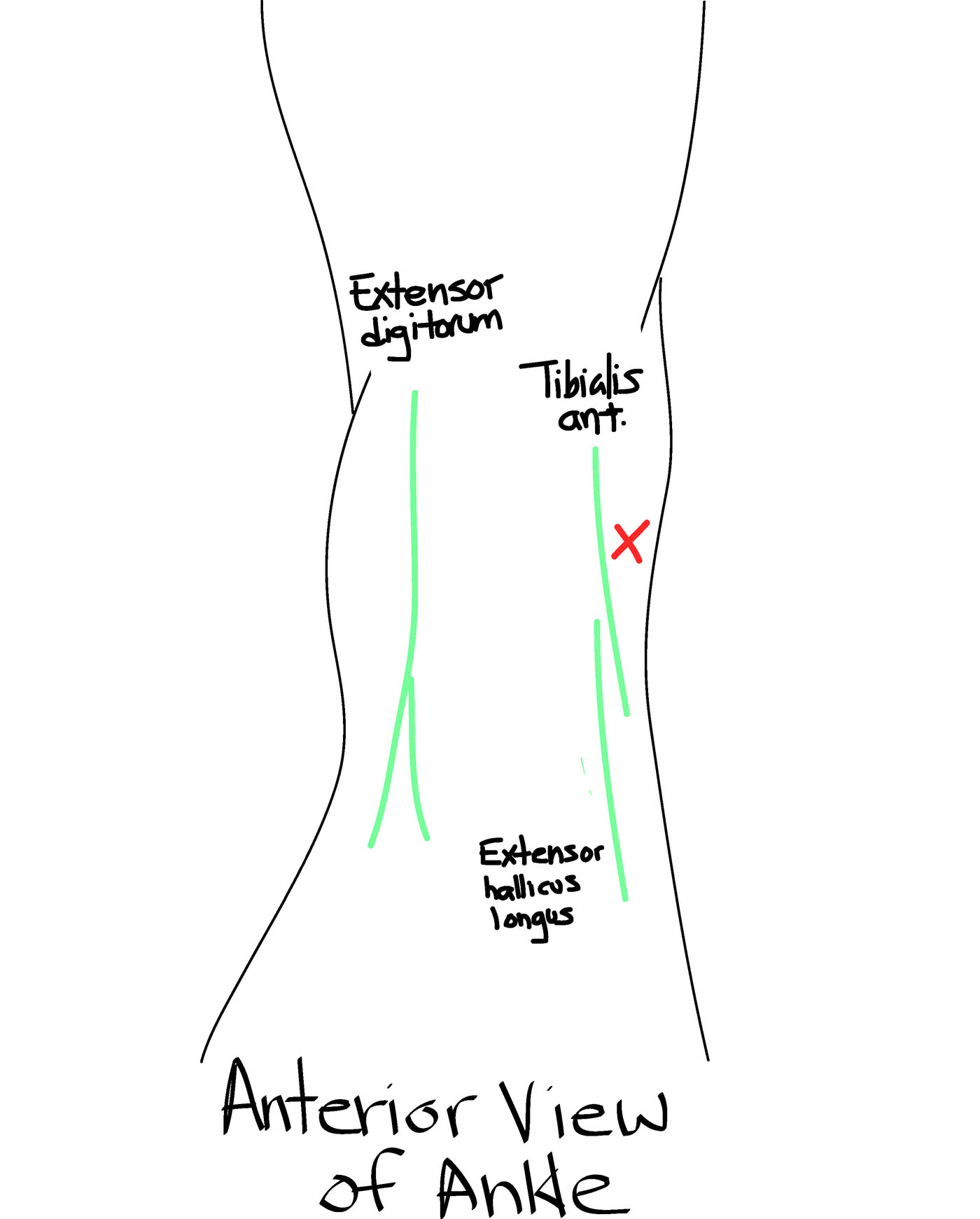
Musculoskeletal: Moving all extremities freely. No swelling or erythema of legs. Normal graded compression of bilateral common femoral vein and popliteal vein.
Skin: Warm and dry. No rashes or mottling.
Psychiatric: Fully oriented. Anxious but interacting appropriately for situation.
I would be glad to hear your feedback. Contact me if your are interest in joining me in my lobbying efforts of ACEP, ABIM, and most importantly CMS.

Yes, agree- this is the future; POCUS conceptually is extension of PE, so why not chart it the same… ?
Yes, I agree. But from the standpoint of the insurance – do you charge extra to use your stethoscope? If it so neatelly integrated in the report, and such an important part of PE that you cannot leave it out – why charge it extra.
Other way it can be done – after writing short PE findings, you write: I also do a POCUS (or whatever you do). And then in a few words summarize findings. Now it s clear it is extension of PE. Results are documented and it is clear for the insurance it is an extra that should be reimbursed. That report is also a kind of an equation from which it is clear how far you got with “old school” pe and what was gained by doing POCUS also. Another clear reason why to reimburse it.
I agree with Andrej and that is the way I do it every day. After PE findings I write findings of the focused US, followed by ECG, lab….And at the end all the key findings are included in the opinion.
Charles
I have been teaching ultrasound for 3 decades. I have seen physicians initially resist, then endorse, then bill, then resist unless able to bill.
To accommodate, our institution developed a cumbersome and draconian system that actively discouraged bedside ultrasound, or it would be performed for free and often undocumented. Both of these are unfair to the physician who developed and maintains an ultrasound skill set, and the patient who may not get an appropriate exam or have an exam go undocumented.
I like your approach, and third party payer must recognize that you deserve compensation for a greater level of care provided than that of your colleague who does the same exam, without ultrasound, and walks away with much greater uncertainty and error.
This is very well said.
Dave Plummer M.D.