Incessant ventricular fibrillation is difficult to manage. The mainstays of treatment include:
- LUCAS CPR and ResQPod impedance threshold device
- Multiple defibrillations
- Amiodarone
- Magnesium
- Lidocaine
- Esmolol
We have previously explored the option of using high energy defibrillations for this situation.
A novel technique which has been discussed in the literature is the stellate ganglion block. The stellate ganglion is part of the sympathetic chain formed by the inferior cervical and first thoracic ganglia, and provides sympathetic innervation to the upper extremities, head, neck, and heart. The procedure can be performed blindly, but usually done under fluoroscopy for reflex sympathetic dystrophy by pain specialists. Direct ultrasound guidance may allow this procedure to be performed with accuracy during resuscitation efforts. By blocking the sympathetic output, to the heart there is the possibility of ceasing the ventricular storm. There is a risk however of residual left ventricular dysfunction.

Figure 1. External landmarks and probe placement for performing an ultrasound-guided stellate ganglion block.
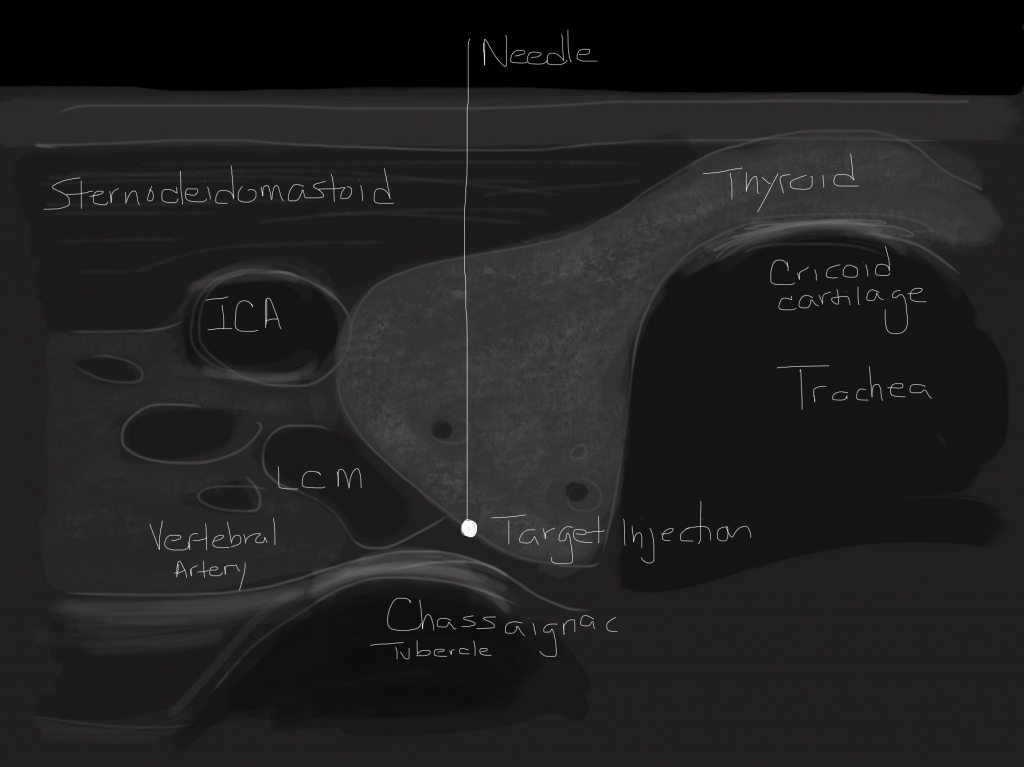
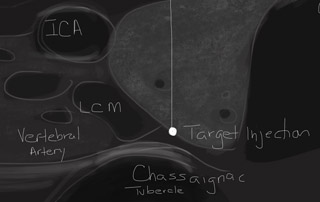
Figure 2. Ultrasound image demonstrating internal structures and needle placement for performing an ultrasound-guided stellate ganglion block.
Equipment
- CHG prep.
- 1% buffered lido with 27 ga 1.5 in needle.
- 25 ga 3.5 in spinal needle.
- 7 cc 1% lidocaine with epinephrine or 0.25% bupivicaine.
- Ultrasound with high-frequency linear probe.
Procedure
- Place patient in supine position with neck extended.
- Palpate to identify the thyroid cartilage and cricoid cartilage. Place a finger in groove lateral to trachea and palpate a bony prominence known as Chassaigniac tubercle. This is the C6 level and should be marked.
- With ultrasound, start in the transverse orientation at the C6 level. Visualize the trachea and cricoid cartilage. Move the probe slightly laterally. Visualize the Chassaigniac tubercle, thyroid.
- Move the probe slightly inferior, until the bony process flattens out.
- Using color Doppler indentify the perforating thyroid arteries, carotid artiery, and verterbal artery.
- Anesthestize the site with lidocaine.
- Advance a 2.5 ga 3.5 in needle through the tract to contact the os at C7. The needle is backed off slightly. Verify no blood return on aspiration to confirm that you are not in a vascular space.
- Inject 6-7 ml of anesthetic.
References
- Circulation 2000;102:742. Treating Electrical Storm–Sympathetic Blockade vs ACLS Guided-Therapy.
- PainMedicine 2011;12:1196. Left Stellate Ganglion Blockade for the Management of Drug-Resistant Electrical Storm.
- TexHeartInstJ 2011;38:409. Left Stellate Ganglion Block for Continuous Ventricular Arrhythmias.
- AnesthAnalg 1994;79:1082. Left Stellate Ganglion Block Impairs Left Ventricular Function.
This intriguing idea was brought to my attention by Dr Brian Driver, EM/IM PGY4, Hennepin County Medical Center.

[…] people have even used stellate ganglion (the source of sympathetic outflow to the thorax) block as a treatment for electrical […]
is the ica at this level. i would have thought it is the cca.
Historically SGB was employed in Pulmonary Embolism too,to improve its clinical distress to the patient…
[…] of Hennepin’s experience with esmolol infusions during arrest that I’ve also used. The stellate ganglion block sounds fascination but I haven’t had the opportunity for that one […]