Cardiac pacemakers and their malfunctions are often daunting for the emergency physician to diagnose and manage. This is the first part of a series covering this area.
- Part 1. Pitfalls and pearls of temporary transvenous pacing.
- Part 2. Procedural instructions for placing a transvenous pacemaker and the use of the temporary pacer generator.
- Part 3. Introduction to permanent pacemakers and ICDs.
- Part 4. Diagnosing problems permanent pacemakers and ICDs.
On to a case for discussion.
A nursing patient was brought to the emergency department for evaluation of lethargy, “being floppy”, and hypotension (90/50 mmHg). He was known to have right-sided systolic dysfunction, medication controlled hypertension, insulin-controlled type 2 diabetes mellitus, and CKD Stage III.
On physical exam he was noted to be obtunded and bradycardic. IV access was established, and initial laboratory tests were sent. He was orotracheally intubated without difficulty and easily ventilated. Atropine was given without an increase in his heart rate. He was placed on transcutaneous pacing. We presumed the patient was suffering from hyperkalemia and he was given calcium gluconate, and shifted with insulin/glucose. It was difficult to establish good capture. Multiple different pad locations were attempted, and eventually we were able to get intermittent capture using a right-parasternal and apex pad location.
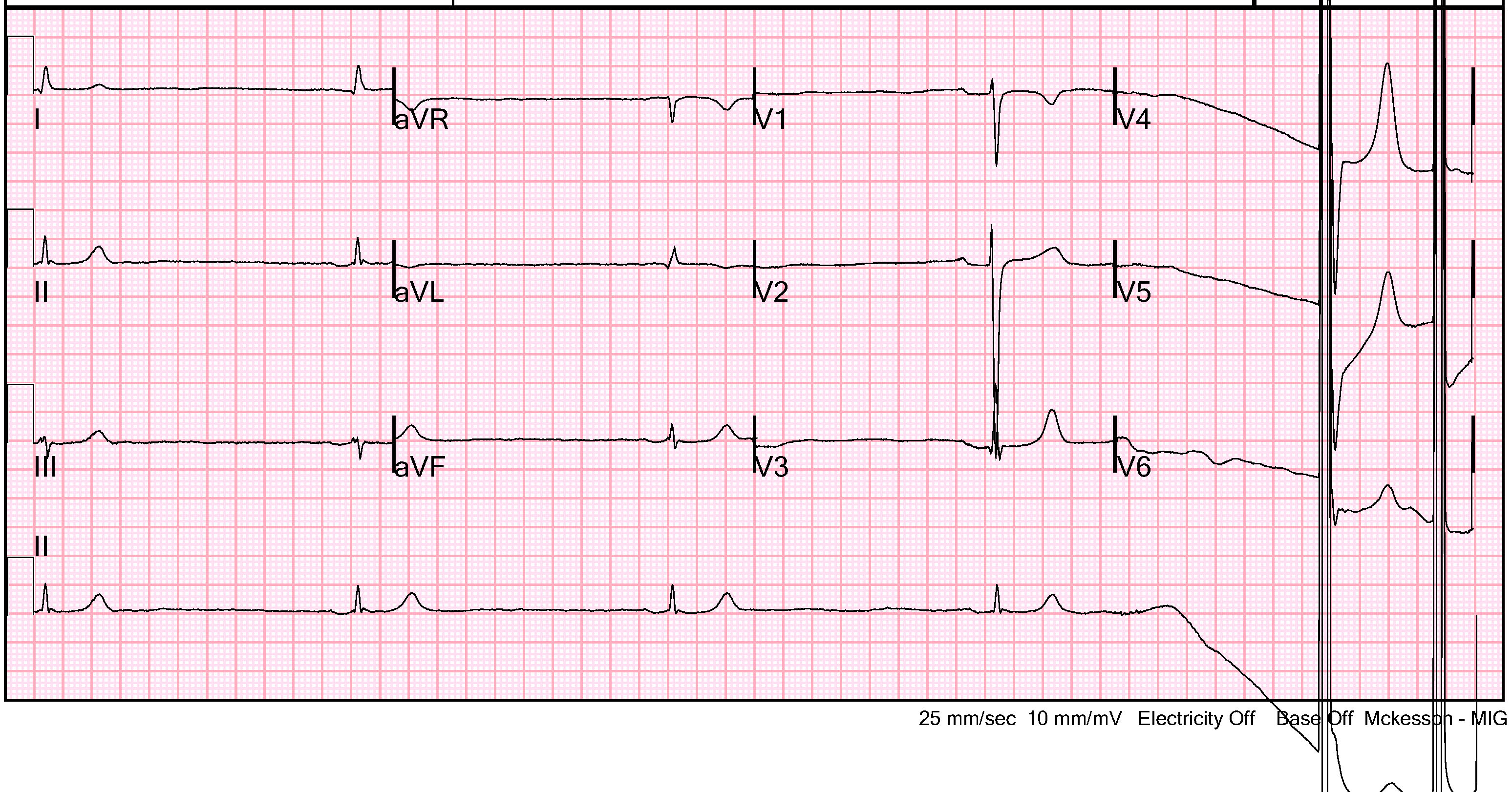
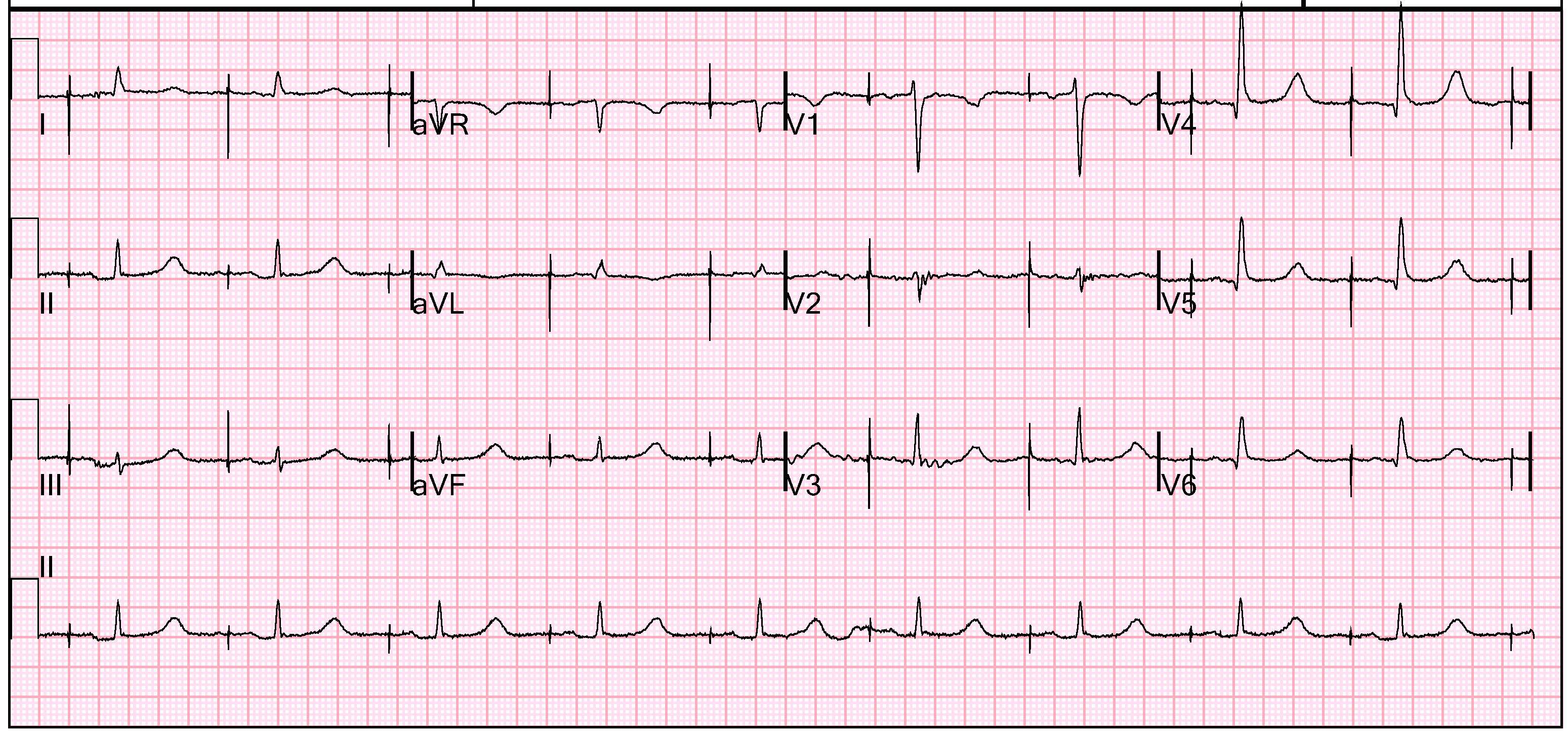
A 12-lead ECG was obtained as shown below. This was interpreted as sinus bradycardia, with a narrow QRS complex and significant T-waves abnormalities. There did not appear to be any ST-segment or T-wave changes concerning for ischemia. The large voltages recorded on the right-side of the strip occurred when the transcutaneous pacer was restarted.
A bedside cardiac ultrasound confirmed bradycardia. Contractility was adequate and there were no gross focal wall motion abnormalities.
The remainder of the FAST exam was was notable for free fluid in the abdomen. This included fluid in Morrison’s pouch, suprapubic region, splenorenal angle, as well as bilateral pleural effusions. This was presumed to be ascites. Evaluation of his IVC while being positively pressure ventilated showed a dilated vessel without significant respiratory variation. Images from the FAST exam and a video clip of the IVC ultrasound are shown below.


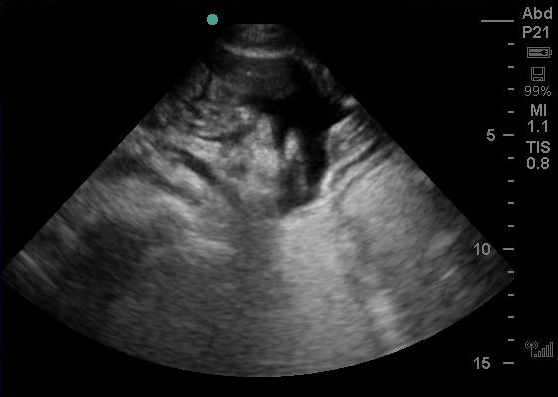
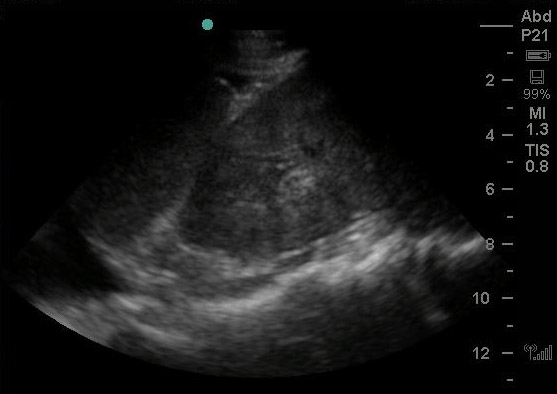
At this point, we got back initial laboratory tests. His blood counts were normal. Chemistry panel revealed a potassium of 7.4 mEq/dl. He was given additional calcium gluconate. Given that the transcutaneous pacing was intermittent, we decided to place a transvenous pacing wire (details of this procedure in Part 2). Below you can visualize the floating balloon in the right ventricle. It is visible as the hyperechoic structure with shadowing that is seen in the right ventricle.
Unfortunately, a chest radiograph and ECG were not immediately obtained in the ED. The patient was admitted to the Medicine ICU, and shortly thereafter was noticed to have only intermittent capture. A supine chest radiograph was obtained, which is shown below.
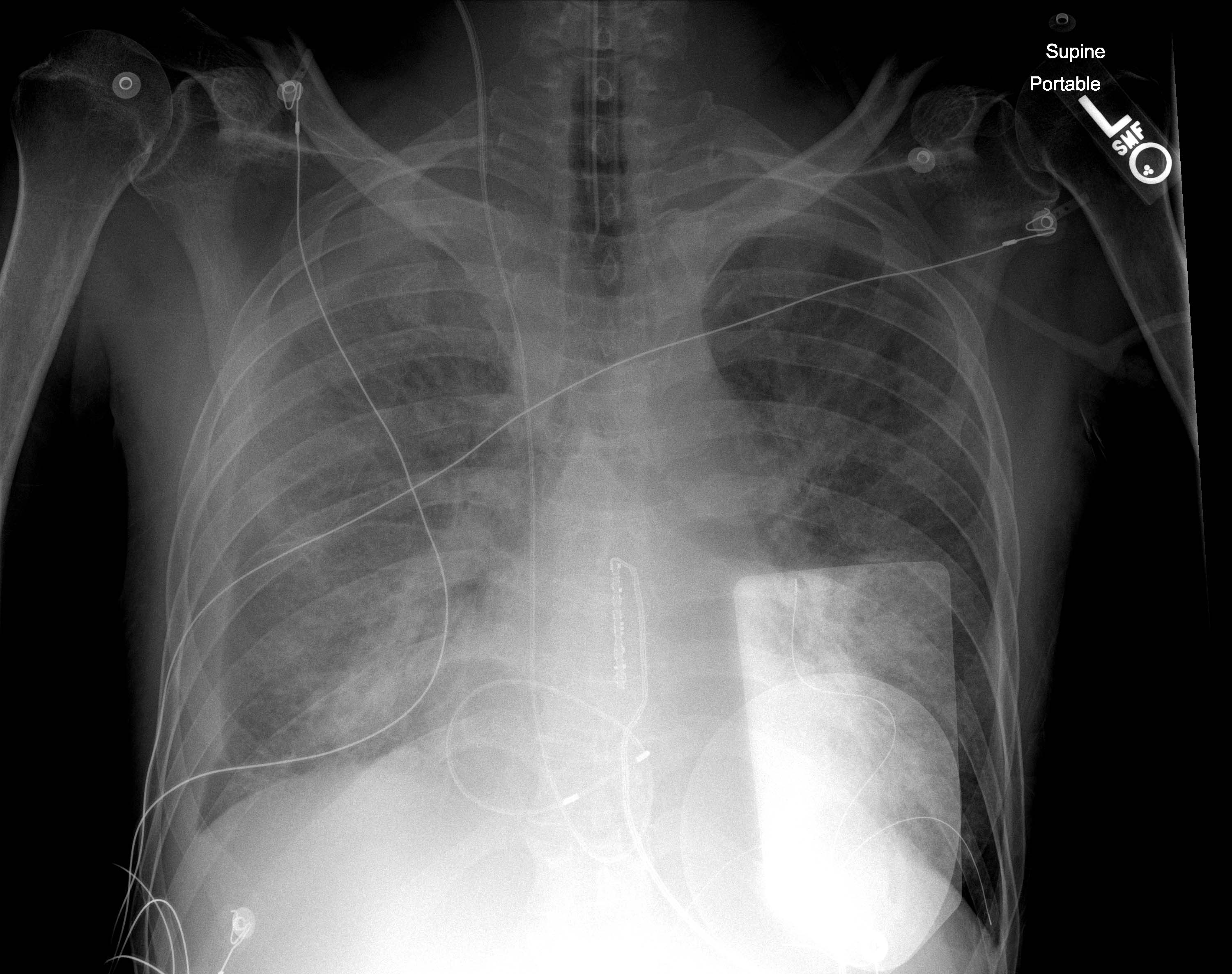
This is a fairly difficulty radiograph to interpret. The pacer pads can be seen over the left hemithorax. The pacer can be seen in the internal jugular vein and descending the SVC to the heart. It is looped in the right ventricle, and there is likely part of the wire that crosses the tricuspid valve. Below is a schematic of the pacer wire to help you interpret the chest radiograph and visualize how the pacer wire was coiled.
The patient was turned for cares, and it was noticed that the morphology of rhythm recorded on cardiac telemetry had changed. A 12-lead ECG while being paced was obtained, and is shown below. As you can see there are pacer spikes prior to each p wave, and there is a narrow QRS complex. The axis of the p wave is inferior and to the left. This is means that the the pacer is atrial pacing, and likely at a location high up the ventricle. It is likely that the pacing tip had been pushed out of the ventricle and was not in contact with the right atrium wall. This was attributed to excessive slack in pacer wire because of the coiling, and a partially inflated floating balloon.
The patient was taken to the cardiac catheterization lab for repositioning of the pacing wire under fluoroscopy. The wire was confirmed to be coiled and almost tied in a knot. The tip was in the atria, and the floating balloon was partially inflated. It was respositioned without difficulty and excellent capture. The patient was returned to the MICU, and ultimately underwent emergent dialysis to correct the underlying hyperkalemia.
Procedures performed in the emergency department are performed on unstable patients under time-critical conditions can have many steps that introduce complications. Familiarity and checklists, can dramatically increase not only their success but also safety.
Cardiac pacing is can be a life-saving procedure. But there are many important lessons. Below are some of the most critical
- Before considering either transcutaneous or transvenous pacing for bradycardia, the patient should be evaluated for significant hypotension and other signs of hypoperfusion. If these are not present, the bradycardia can be observed.
- The floating balloon should be fully deflated.
- Remember that bradycardia is not always a primary cardiac issue such as sick sinus syndrome, atrioventricular block, or myocardial ischemia. Always consider secondary causes such as hyperkalemia, hypothyroidism, hypothermia, or overdose with beta-blockers, calcium channel blockers, digitalis, clonidine, or other antiarrhythmics.
- The right internal jugular vein is optimal for placing the transvenous pacer.
- Typically the pacer wire should be placed to a depth of about 40-45 cm if entering from the right internal jugular vein. It should be pre-measured on the patient before insertion.
- The manufacturer instructions and standard practice by the electrophysiologists are to use air in the floating balloon. There are case reports of the balloon rupture causing air embolism, most kits come with an inflation syringe that limit the amount of air to 0.75-1.0 cc. The use of saline can interfere with balloon deflation, and at least anecdotally makes it harder to float into place.
- The balloon should be fully deflated once properly positioned and achieving good capture.
- As you are placing the pacer wire, the patient should be monitored on continuous cardiac monitoring. Successful cardiac pacing with a properly placed pacing wire should demonstrate ventricular pacing with a LBBB morphology.
- An ECG and chest radiograph should be obtained immediately after placing the transvenous pacer wire and obtaining capture.
- The chest radiograph should be inspected for the path of the pacer wire. There should be no lops or coiling, and the pacer tip should seated in the apex of the right ventricle.
- The initial amperage should be set to 25 mA. Once capture has been achieved, this should reduced until you loose capture, and then doubled. Typically this is around 5 mA.
- The rate should be set at an adequately level to avoid hypotension, usually around 60 bpm.
- If the patient is poorly tolerating transcutaneous pacing, an alternative to transvenous pacing would be to intubate and sedate the patient.
- After any cardiac pacing whether transcutaneous or transvenous, when the pacing is removed there is a significant risk of asystole.

[…] ERCast (Torsade de Points) + Ultrasound Podcast (transvenös pacing): Joe Bellezzo från ED ECMO pratar om behandlingsstrategier för TdP med temporär pacing, samt hur det går till i praktiken. Väldigt proaktivt perspektiv på handläggning och en del fallgropar. För mer info om transvenös pacing rekommenderas också ett lite äldre inlägg från Resus Review. […]