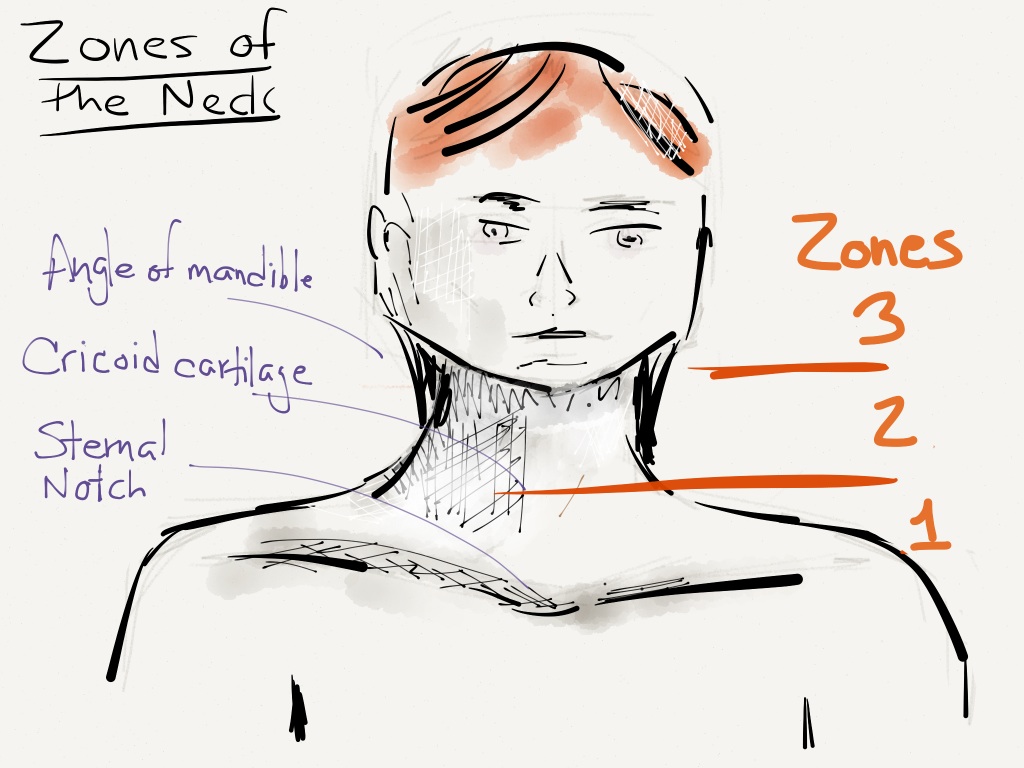
Zones of the Neck
- Defined by mandible, cricoid cartilage, and sternal notch.
- Most injuries sustained in Zone II, especially carotid injuries
- Zone I mortality high due to intrathoracic injuries.
- Posterior triangle with few vital structures. Important exception is subclavian at risk just above clavicle.

Rapid Assessment
- Speak (voice change: hoarse, dysphonia)
- Cough (hemoptysis)
- Swallow (dysphagia)
- Carotid auscultation (bruit, thrill)
- Symmetric pulses
Penetrating Trauma
- Based on the Eastern Association for the Surgery of Trauma (EAST) Guidelines
- Unstable: Surgical exploration
- Stable: CTA initial study of choice all zones and blunt
- C-spine immobilization not required for isolated penetrating trauma if patient awake and neuro intact1.
1. Arterial injury
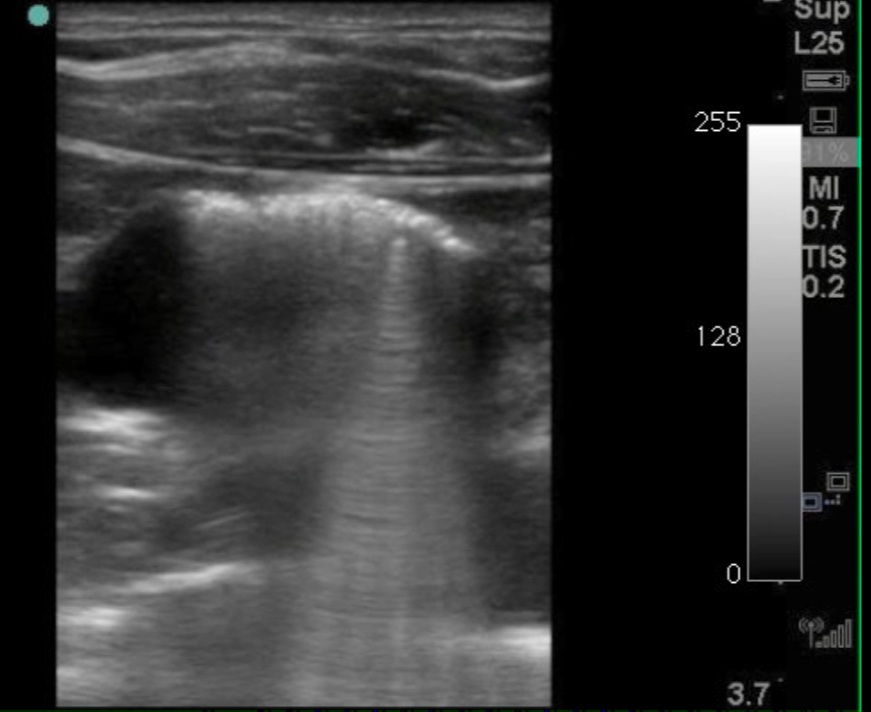
- CTA or US in Zone II
- US up to 100% Sn & Sp for arterial injury
- Angio if positive or inconclusive (s.a. streak artifact)
- IR can diagnose and embolize (esp Zone III)
- Noncontrast CT sufficient if trajectory remote to vessels
2. Laryngeal injuries
- – Direct laryngoscopy for suspicious wounds
- – CTA
3. Esophageal injuries
- Not excluded by normal x-rays
- Contrast esophagoscopy or esophagraphy (Gastrografin → Barium → Endoscopy)
- Typically done after resuscitative phase
Blunt Neck Trauma
1. Cerebrovascular injuries
- Any neurologic abnormality not attributable to other injuries
- Suspected arterial epistaxis
- High risk head trauma
- US not adequate, CTA is study of choice
2. Esophageal injuries
- Very rare and evaluation only required for symptoms
Contribute your thoughts.