The Rise of Prone Positioning
Prone positioning has transitioned from a salvage procedure for ARDS, to a more routine part of the armamentarium (including , neuromuscular blockade, inhaled prostacyclin, APRV) based on the dramatic success seen in the study by Claude Guérin published in the New England Journal of medicine in 2013. In this trial involving 466 patients, a mortality benefit of over 50 % was seen at 28-days and 90-days.
Prone positioning improves lung compliance and ventilation-perfusion matching by reducing the posterior atelectatic lung. This is because the heart and anterior lung fields are placed down, instead of acting with gravity to compress the larger posterior lungs. Therefore, more of the lung parenchyma is ventilated, and at a fixed tidal volume the lung will suffer less barotrauma.
Placing a patient in the prone position requires significant effort and has serious risks. Close attention to lines, drains, and airway is critical, as is obsessive attention to pressure point padding and prevention of ulcers. Because of the “unnatural ICU position”, and the risks involved, ICU staff (physicians, nurses, respiratory therapists) have a natural reluctance for prone positioning despite its potential benefits.
Pre-Prone Planning
Should be considered a procedure, with planning, consent, and timeout. Since prone positioning is usually considered are ventilator optimization, inhaled prostacyclins, deep sedation and neuromuscular blockade have already been done, the patient is often has poor oxygenation, and tenuous respiratory and cardiovascular condition. Given the risks, careful planning and preparations are critical.
- Identify physician to authorize and supervise procedure (attending or fellow).
- Order for prone positioning should be entered into the patient’s chart.
- Review inclusion & contraindications.
- Discuss risk/benefits of the procedure with the patient’s decision maker.
- A central venous catheter, arterial catheter, urethral catheter, and feeding tube should be placed before proning.
- Gather staff that will be available for the 15-20 minutes to perform the proning. This usually involves 3-4 nurses, physician, and respiratory therapist.
Gather Equipment Required for Proning
- Pillows (3-4).
- Flat sheets (2).
- Dry flow pads (2-3).
- ECG leads/patches.
- ETT holder (twill tape, E-tab, etc).
- Extra ventilator circuit including suction catheter.
- Doughnut pillow for head.
- Ensure oral suction and ETT suction available (either inline or catheter).
- Have emergency airway cart and appropriate sized ETT immediately available.
- Consider ordering speciality bed.
Pre-Proning Preparation
- Verify ETT is well secured.
- Optimize ventilator settings and pre-oxygenate patient. Place patient on FiO2 100% during turn.
- Suction ETT and oral cavity.
- Remove and cap unnecessary lines tubes (eg, blood pressure cough, CVP monitoring, tube feedings, maintenance fluids).
- Clean patient.
- Perform any necessary wound care and change dressings.
- Ensure patient is well sedated, with adequate analgesia and neuromuscular blockade.
- Remove ECG patches and leads from limbs and anterior chest.
The Turn Checklist
- MD in room.
- Identify turn leader (usually the patient’s primary nurse).
- Respiratory therapist at head of bed. Responsible for ETT
- Minimum 2 staff each side of bed.
- Tuck arm under patient (arm closest to the ventilator)
- Place oximeter probe on limb not being turned under patient.
- Place two pillows on patient’s chest.
- Place flat sheet on top of pillows/patient.
- Slide patient to edge of bed (away from ventilator)
- Check ETT, lines, tubes.
- Rotate patient and slowly turn toward vent until in prone position.
- Check ETT, lines, tubes. Assess lines and tubes for dislodgement/kinks/air entry
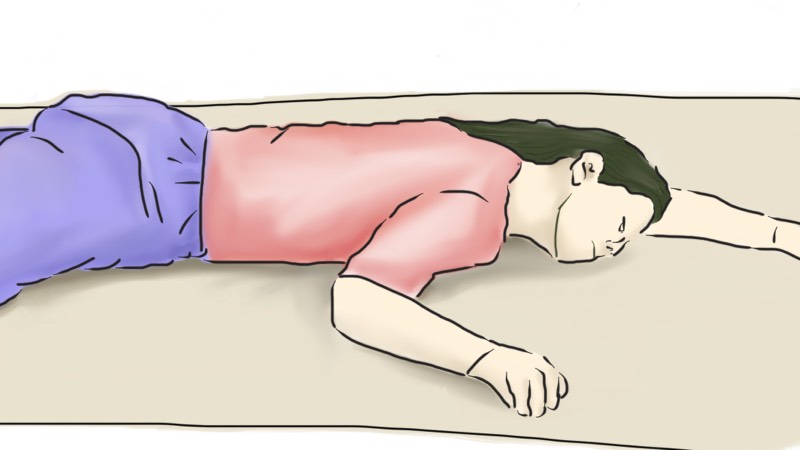
- Position arms in modified swimmers crawl. Face is in the direction of the raised arm. Shoulder dropped and elbow below axilla and other arm at side, palm facing up (see figure above).
- Ensure pillows are under shins and toes are off the bed.
- Reattach disconnect lines/cables.
- Place bed in reverse Trendelenburg.
- Reassess ETT cuff pressures, tidal volumes, sats, BP, HR.
I recommend that initial proning be performed manually a regular patient bed to monitor the response. We have been maintaining the patient in the prone position 16 hours/day and placed in the supine position for 8 hours per day assuming the patient can tolerate it. If it appears that the patient is going to require ongoing proning, there is benefit from safety and staff resources to using a speciality rotating bed.
Learnt alot from this piece of article.
Newton @Kenyatta University School of medicine
Do you place the ecg patches in the same order as when you do when the patient is supine; white and green on the right while black and red are on the left? With the recent flu season hitting us so hard we are proning several people in my Icu due to ARDS.
Nice lesson