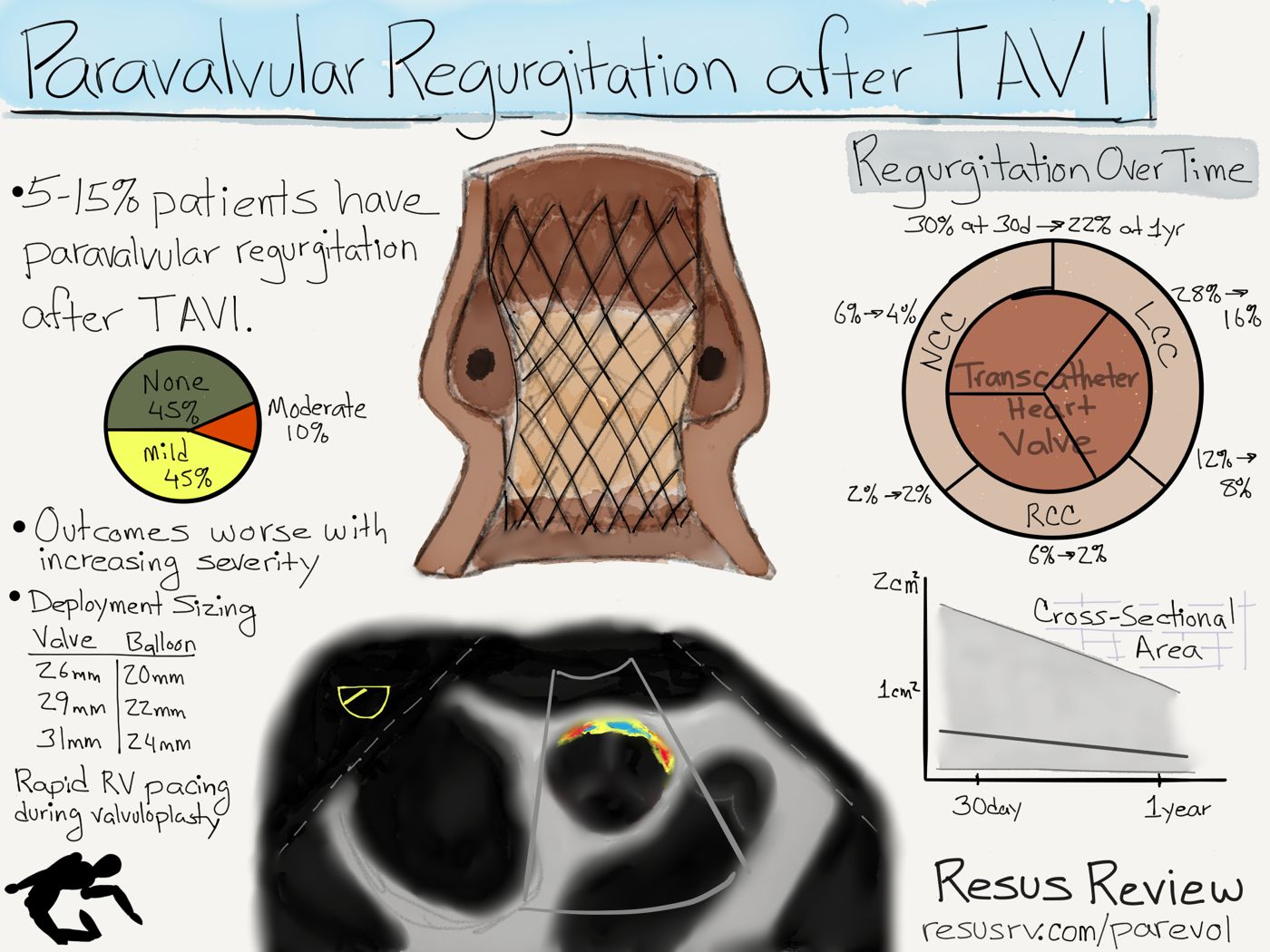
An common complication following transcatheter aortic replacement is paravalvular regurgitation (PAR). Mild to moderate regurgitation occurs in over 50% of patients. The 1 year mortality of patients after TAVI correlate with the severity of the regurgitation.
Aortic Valve Changes after TAVI
Transcatheter cardiac interventions are a fast evolving field. Aortic valve intervention is usually performed for aortic stenosis. Transcatheter aortic valve implantation (TAVI, TAVR) has shown to improve valve area from 0.7 cm2 to 1.7 cm2. This is associated with an decrease in the gradient from 45 mmHg to 7 mmHg. Not unexpectedly, this often provides substantial symptomatic relief for patients.
TAVI Paravalvular Regurgitation
Regurgitation is caused by deployment problems and anatomic issues.
- Valve size used relative to the anatomy
- Balloon size used for the valvuloplasty
- Depth placement within the valve
- Calcification of the native valve
- Native valve leaflet entrapment
- Dilation of the supravalvular aorta
2-dimensional transthoracic echocardiography (TTE) is convenient for for assessing paravalvular regurgitation, but does not provide adequate quantification and spatial resolution. Transesophageal echocardiography (TEE) overcomes these barriers at the expense of requiring an invasive procedure. Angiographic supravalvular injection and hemodynamic measurements can also provide functional estimates of regurgitation.
The maximum regurgitation tends to occur between the intersection of the noncoronary cusp and along the left coronary coronary cusp.
With hemodynamically significant regurgitation, a postdilation can often significantly reduce paravalvular regurgitation without increased risk of stroke or permanent pacemaker placement.
Regurgitation Changes During 1 Year
Overtime, most the paravalvular regurgitant jets decrease, and some disappear completely. The cross-sectional area of the regurgitation typically decreases about 45% (0.36 cm2 to 0.12 cm2). This is reflected in the decrease of involved perimeter which decreases a similar 43% (8.2 mm to 4.7 mm).
With evolution of deployment technique, valve sizing, use of balloon valvuloplasty, and use of computed-tomography procedure planning, the rates of paravalvular regurgitation can be decreased.
Selected Key Readings
- Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011;123:299.
- Toggweiler S, Humphries KH, Lee M, et al. 5-year outcome after transcatheter aortic valve implantation. J Am Coll Cardiol. 2013;61:413.
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. NEJM 2011;364:2187.
- Abdel-Wahab M, Mehilli J, Frerker C, et al. Comparison of balloon-expandable vs self-expandable valves in patients undergoing transcatheter aortic valve replacement: the CHOICE randomized clinical trial. JAMA. 2014;311:1503.
- ■ Genereux P, Head SJ, Hahn R, et al. Paravalvular leak after transcatheter aortic valve replacement: the new Achilles’ heel? A comprehensive review of the literature. J Am Coll Cardiol. 2013;61:1125.
- Toggwiler S, van Shie B, et al. Natural Course of Paravalvular Regurgitation After Implantation of the Self-Expanding CoreValve: Insights rom Serial TEE Measurements. J Invas Cardiol 2015;27(9):435.
- Zoghbi WA, Chambers JB, Dumesnil JG, et al. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves. J Am Soc Echocardiogr 2009;22:975.
[…] not without its own set of complications, it offers benefits for patients who may have gone without treatment when surgery was the only […]