Evaluation of pediatric head trauma, especially the decision to obtain advanced imaging has significant risk/benefit trade-offs. Three major studies have been performed to aid the emergency physician and parents in this decision.
CATCH
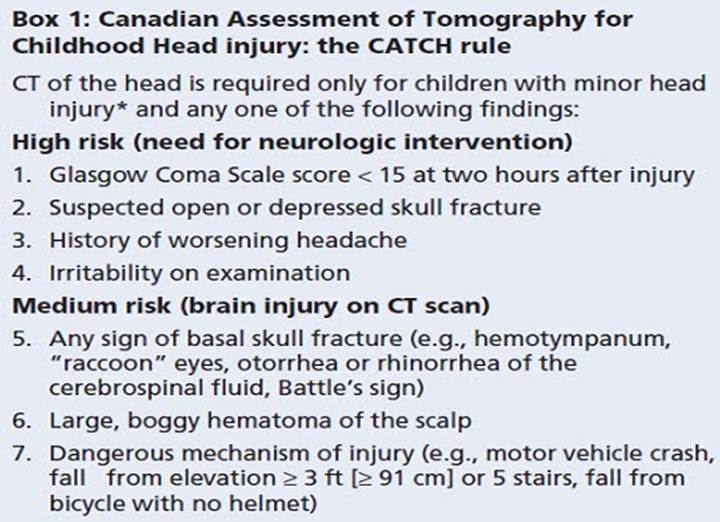
- Canadian Assessment of Tomography for Childhood Head Injury
- CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury. Osmond et. al. CMAJ. 182(4) 341-348, 2010
- Objective: Prospectively Derive an accurate and reliable clinical decision rule for the use of CT for children with minor head injury
- Enrolled 3866 pts from 10 Canadian hospitals with 7% being less than 2 years of age
- Inclusions
- < 16 yo
- Presenting within 24 hrs
- Blunt trauma resulting in LOC, amnesia, witnessed disorientation, persistent vomiting (2 episodes 15 minutes apart) or persistent irritability (under 2 yo)
- Initial GCS of at least 13
- Exclusion
- Penetrating trauma, depressed skull fx, focal deficits, development delay or suspected abuse
- Methods
- ED providers evaluated pts for 26 standardized clinical findings from history, general exam and neurological status.
- Potential predictor variables were selected prior to initiation of trial via literature and pilot study
- Recursion partitioning was used to combine variables to find best combination of predictor variables that were highly sensitive for detecting the outcome measure.
- All those d/c without CT had 14 day telephone f/u.
- Primary outcome: Was need for NSG intervention
- Secondary outcome: Evidence of brain injury on CT.
- Results
- Having any 4 of the high-risk factors predicting outcome of NSG intervention had a sensitivity of 100%
- The presence of any of the 4 high-risk factors or 3 medium-risk factors in the rule would identify any CT-visible brain injury with a sensitivity of 98.1% (3 missed cases) (NPV 99.8)
- 3 missed cases not identified by decision rule were an occipital skull fracture with small pneumocephalus, mild brain edema and small EDH. None required treatment
 CHALICE
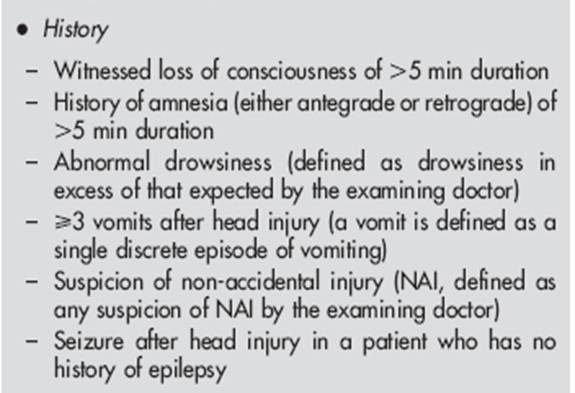
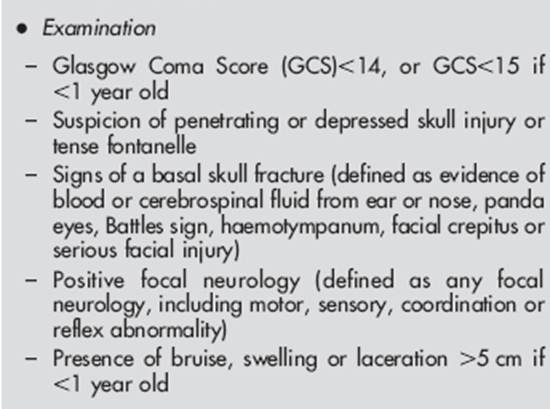
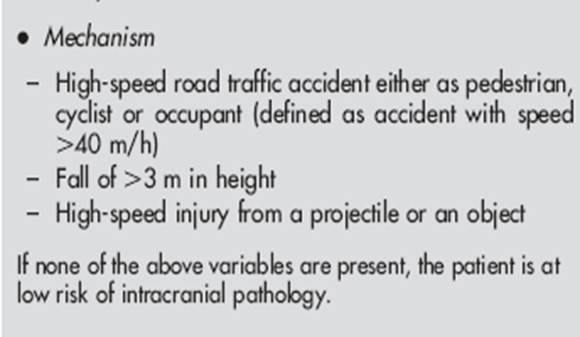
CHALICE
- Children’s Head Injury Algorithm for the Prediction of Important Clinical Events * Derivation of the children’s head injury algorithm for the prediction of important clinical events decision rule for head injury in children. Dunning et. al. Arch Dis Child 91, 885-891, 2006.
- Objective: Derive a sensitive clinical decision rule for the management of children with an acute head injury, which would identify children at high risk so as to undergo CT and allow remaining patients to be d/c.
- Enrolled 22, 772 pts from 10 hospitals in England
- Inclusions
- Any pt with history or sign of injury to the head
- Exclusion
- Refusal to consent
- Methods
- ED providers evaluated pts for 40 standardized variable including mechanism of injury, signs and symptoms.
- Potential predictor variables were selected prior to initiation of trial via literature and pilot study
- Recursion partitioning was used to combine variables to find best combination of predictor variables that were highly sensitive for detecting the outcome measure.
- Primary outcome: Was composite comprising death from head injury, NSG intervention or abnormality noted on head CT.
- Secondary outcome: Presence of a skull fracture or admission to hospital.
- Results
- Overall sensitivity of 98%. (NPV 99.9%)
- Missed 4 patients.
- 2 had depressed skull fractures missed on examination of 1st physician (Assume treatment?).
- 3rd presented after fall against a wall discharged then represented with vomiting 2 hrs later and found to epidural needing needed treatment
- 4th fall from a swing into a stream, returned 11 days later with continued headache and skull fracture. No treatment

PECARN
- Pediatric Emergency Care Applied Research Network
- Identification of children at very low risk of clinically important brain injuries after head trauma: a prospective cohort study. Kupperman et. al. Lancet. 374 (3), 1160-1170, 2009
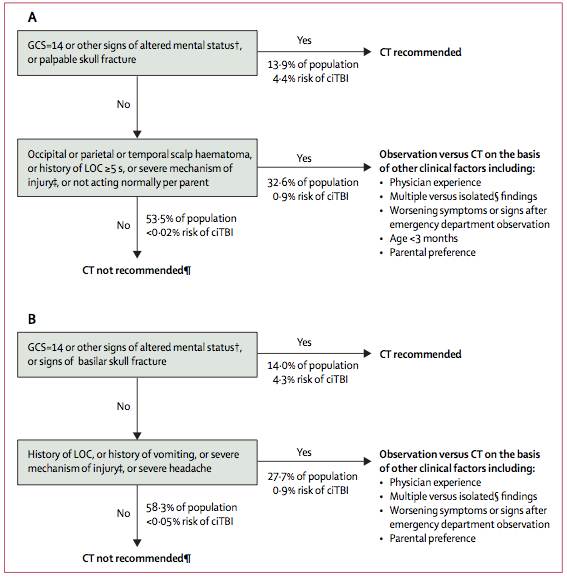
- Objective: Derive and validate prediction rules for ciTBI to identify children at very low risk of ciTBI after blunt head trauma for whom CT might be unnecessary (included separate rule for <2 yo)
- Enrolled 43,904 pts from 25 US hospitals with 25% being less than 2 years of age
- Inclusions
- < 18 yo
- Presenting within 24 hrs
- Exclusion
- Trivial injuries – ground level falls, walking/running into stationary objects (mild injuries) & no signs or symptoms of head trauma other than abrasions and lacerations
- Penetrating trauma, known tumors, pre-existing neuro d/o, shunts, bleeding d/o GCS < 14
- Methods
- Evaluated injury mechanism
- Clinical variables
- Rule derivation was determined by binary recursive partitioning….. ie decision tree
- Preverbal (< 2yo) and verbal (>2yo) children were analyzed separately b/c of young pts greater sensitivity to radiation, decreased ability to communicate, and different mechanism and risks for TBI.
- Decision predictors <2yo
- AMS
- non-frontal scalp hematoma
- LOC > 5 sec
- severe injury mechanism
- palpable skull fracture
- not acting normally according to the parent.
- Decision predictors >2yo
- AMS
- Any lOC
- Hx of vomiting
- Severe injury mechanism
- Clinical signs of basilar skull fracture
- Severe headache
- Results
- For pts < 2 yo — NPV 100% (1176/1176) and sensitivity of 100% (25/25)
- For Pts > 2 yo — NPV 99.95% (3798/3800) and sensitivity of 96.8% (61/63)
- Prediction rule missed 2 unhelmeted biker/inline skater –both large frontal hematoma and “moderate headache”? Neither required NSG
- Believe PECARN to be most useful
- Validated
- Large study 44,000 US pts
- Included different decision rule for children < 2
- Fairly simple rules

[…] Summary of the Major Pediatric Head CT Rules […]
[…] Read the original post: Resus Review – Summary of the Major Pediatric Head CT Rules […]