This 59-year-old gentlemen presented with 3 hours of severe upper sternal chest pressure that radiated to his throat which he described as “strangulating”. No previous cardiac history.

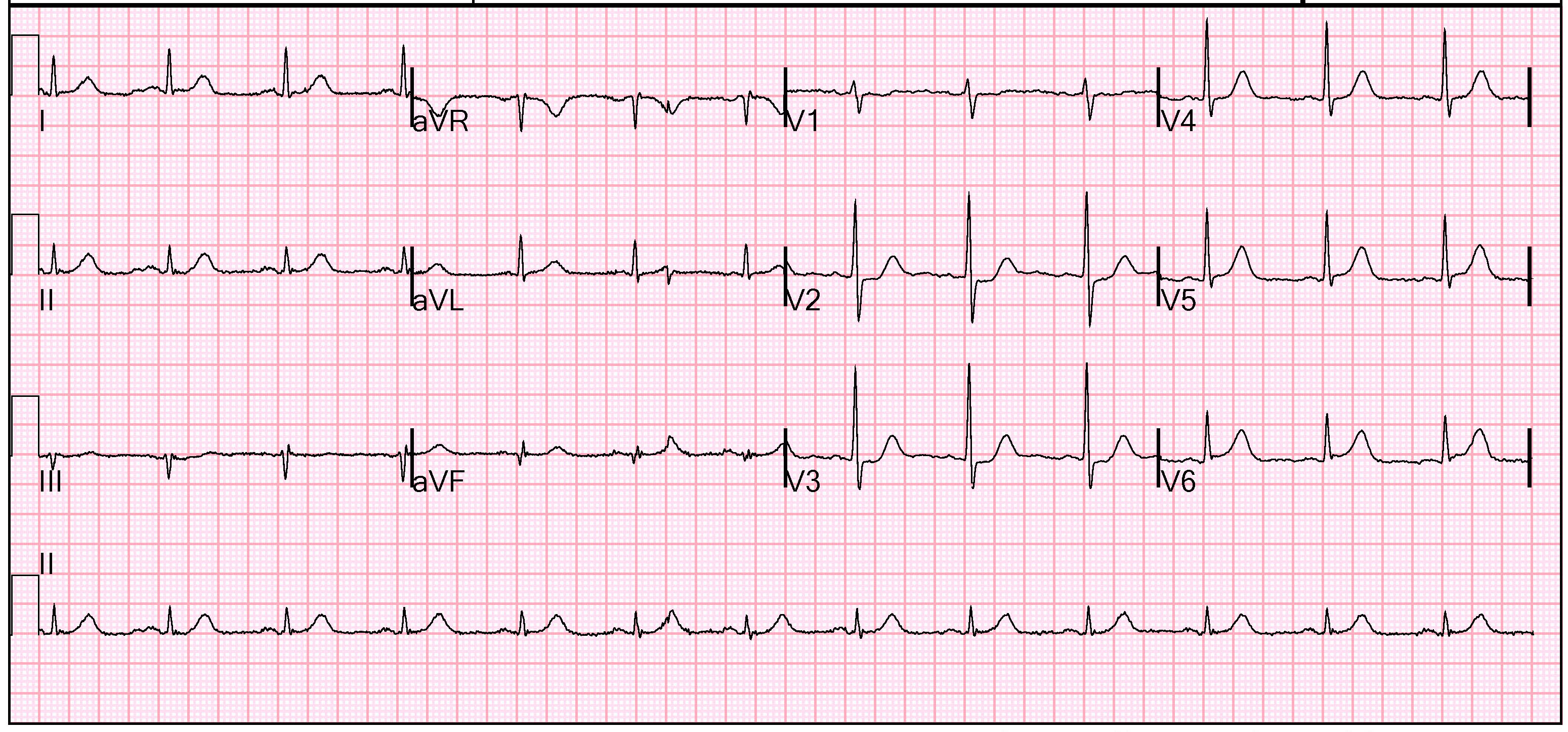
The initial ECG was concerning concerning for ST depression in V2 and V3, with ST-elevation suggested in V5 and clearly seen in V6. This is consistent with a posterior MI. A posterior ECG was obtained about 5 minutes later.
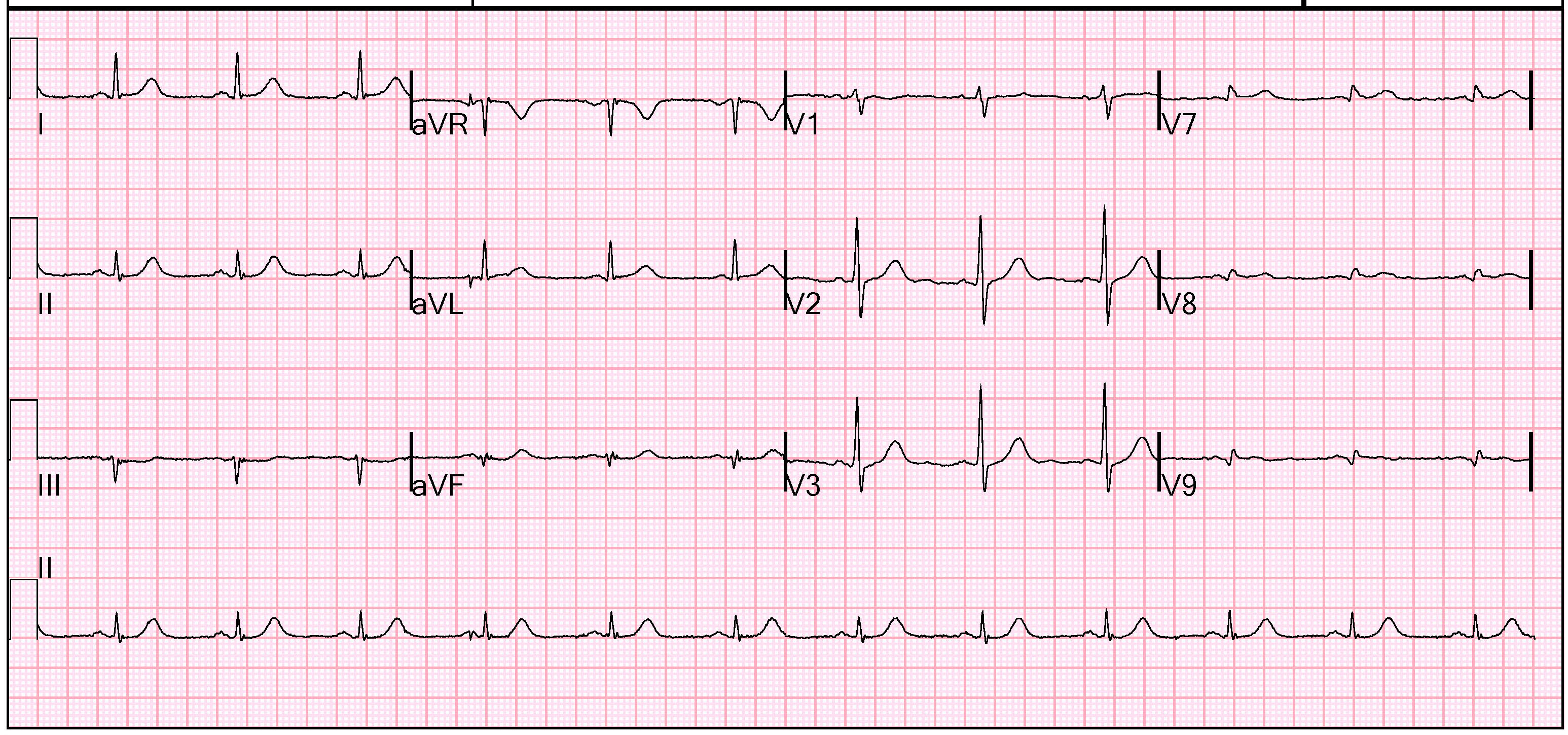
There is low voltage across leads V7-V9, and a large T-wave in proportion to the R-wave, but there is no ST-elevation. Interestingly the ST-depression in V2-V3 is resolving. Dynamic changes like this confirm ACS.
A bedside echo provided difficult visualization, but with Definity contrast a formal echocardiogram confirmed a large posterior wall motion abnormality.
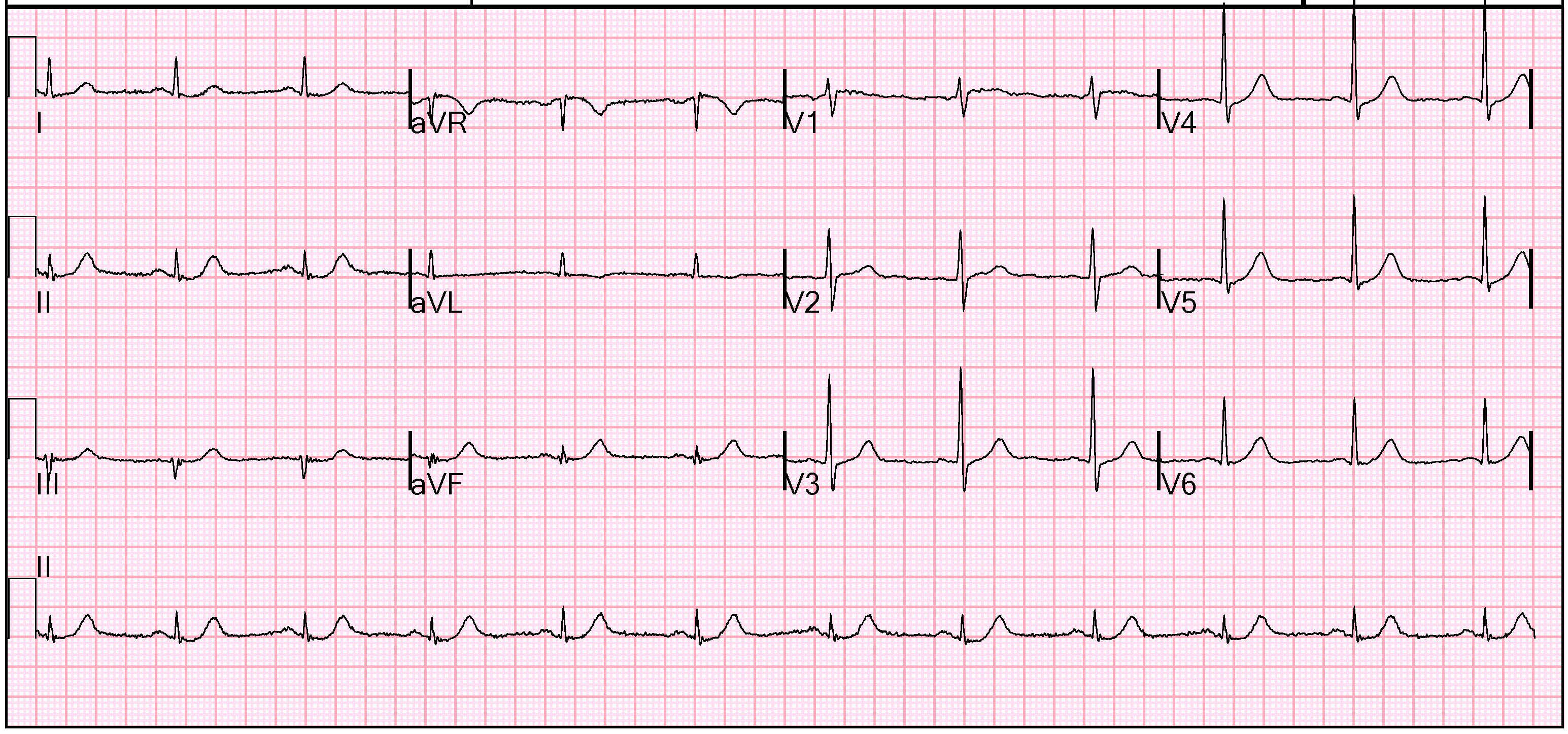
A repeat ECG 45 minutes after the initial one interestingly shows further dynamic ST-segment changes in the precordial leads and dynamic T-wave changes inferiorly.
The patient was brought emergently to the Cardiac Catheterization Lab and he was found to have 99% stenosis in the proximal segment of the 1st OM that gives rise to a good sized lateral branch. He was also found to have a 90% ulcerated plaque in the proximal RCA. The LCX lesions underwent thrombectomy, and both lesions were stented with a drug-eluting stent.

This STEMI was picked up through a combination of ECG and immediate bedside ECHO and the patient went straight to angiography. Up here in Broome (remote NW Western Australia) we don’t have the last option and often not the second option either. Would anyone thrombolyse this chap solely on the ECGs pictured here? I don’t think I would have wanted to.
The second ECG shows evidence of reperfusion, so I would not give thrombolytics. However, I would give Aspririn, NTG, antithrombotics, thienopyridines, a GP IIb IIIa inhibitor and then ship out.
Steve Smith