There are congenital variations from the normal coronary artery anatomy that have significant clinical importance. There are many permutations of the origin site and course of the three primary coronary arteries (left anterior descending, left circumflex, and right coronary artery). The most clinical significant variations include:
- Single coronary artery originating either from the left or right sinus of Valsalva.
- Left main coronary artery or LAD originating from the right sinus of Valsalva.
- Anomalous left coronary artery originating from the pulmonary artery.
If the anomaly has the left main or left circumflex artery coursing between the aorta and pulmonary artery, then external compression of the vessel can occur resulting in myocardial ischemia, syncope, and sudden cardiac death. The obstruction may also result from the intramural course and acute angle of takeoff. Symptoms are worsened by exertion because there is dilation of the aortic root with increased cardiac output.
Origination of coronary vessels from the pulmonary artery is especially troublesome. The pulmonary artery has a low perfusion pressure and carries deoxygenated blood which results in hypoperfusion of the myocardium.
A much rarer condition can occur with anomalous origin of the right coronary coronary artery from the left main, a single left coronary artery, or directly from the aorta in the left sinus of Valsalva. The RCA the course to the right between the aorta and pulmonary artery which subjects it to the same extra-luminal compression and resulting myocardial ishcemia and increased risk of sudden cardiac death.
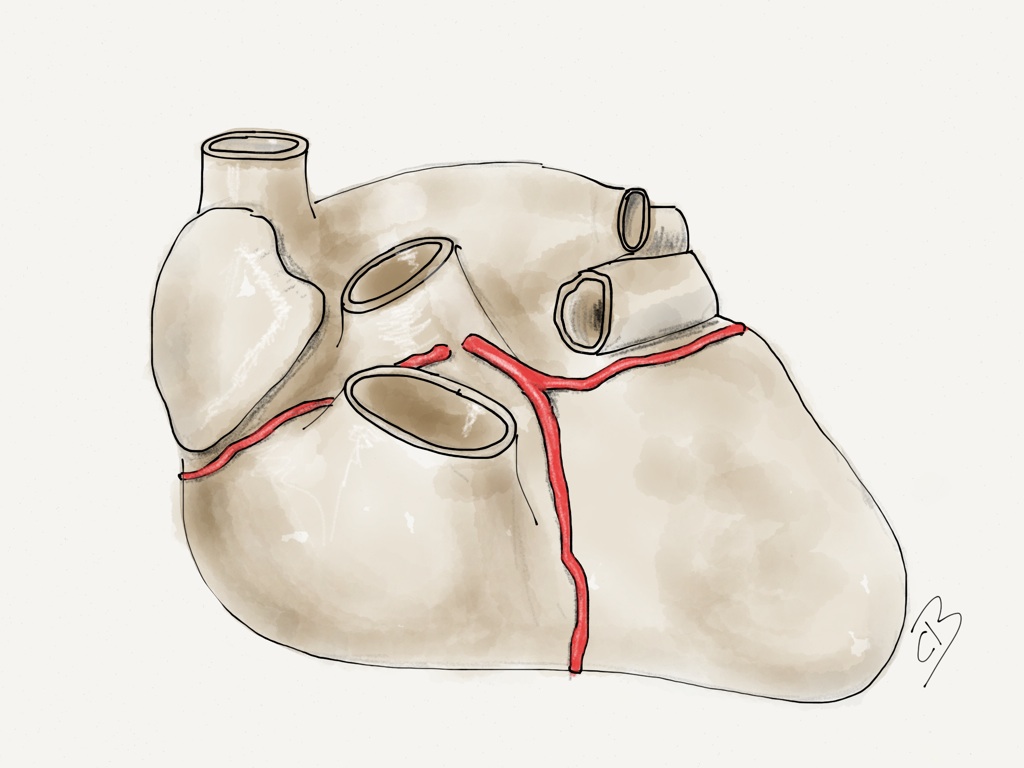

In contrast, origination of the left circumflex from the right sinus of Valsalva is well tolerated because it tends to course behind the aorta rather than between the aorta and pulmonary artery. It generally has no clinical significance.
References
- Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992; 20:640.
- Lorenz EC, Mookadam F, Mookadam M, et al. A systematic overview of anomalous coronary anatomy and an examination of the association with sudden cardiac death. Rev Cardiovasc Med 2006; 7:205.

My healthy 22-year-old son was simply standing in his room and went in to cardiac arrest. The ONLY reason he is alive today is because is friend was with him… a friend who went through EMT training in high school and knew CPR. The EMT’s had to paddle him three times to start his heart. Not only did he survive this, but did not suffer any brain or neurological brain damage. LONG story short, he had an anomalous right coronary artery that came off the left cusp. Our surgeon was able to unroof the right coronary artery several weeks ago. My boy was labeled a miracle. We are still trying to wrap our brains around everything that happened last month.
Thank you for sharing your son’s incredible story. I am so glad he is doing well.
The good outcome is a testament to his friend’s quick thinking and knowledge of CPR. The survival of cardiac arrest depends tremendously on receiving early chest compressions by standers. Thank you for spreading the word.
I am 43 years old. I had V Tach with a HR of 260 occur when running. I have had an ICD placed and was shocked again trying to surf. I am scheduled for an “unroofing” of my RCA.
You are blessed to still be here. God Speed. Once done, you’re in the clear. ?
My daughter, Elsie Caroline, was born with a heart murmur in 2003. Thankfully, it was determined to be a virtually benign condition, attributed to a VSD. However, upon diagnosing the heart murmur in my 2 day old, our new best friend, pediatric cardiologist, Dr. Luke Bruns, found a Right Coronary Anomoly. Which, had it not been for the unrelated heart murmur, would have gone asysymtomatic, and undiagnosed, until the worst case scenario. We all know that, sudden cardiac death. After 9 years of spectactular care and annual EKGs and Echos by Dr. Luke Bruns, Elsie had her “unroofing” surgery performed by the best of the best, Dr. Andrew Fiore, at Cardinal Glennon Children’s Hospital, in St. Louis. Today she is a healthy, thriving, adorable, preppy, monogram & Lilly loving, thirteen year old pain in the ass. Thank God!
Thank you, Dr. Bruns, Dr. Fiore and everyone at Mercy and Cardinal Glennon.