Globe rupture is a serious injury and requires immediate medical attention. Sometimes globe rupture is obvious. The eye can be misshapen with uveal tissue prolapsing out of an anterior scleral or corneal wound. Other times, there may still be an identifiable foreign body present. With ocular ultrasound becoming more common in the ED, our Ophthalmology colleagues have expressed concerned that the ultrasound and repeated evaluations may apply excessive pressure to the globe causing further damage (which I disagree with have manuscript in preparation).
Globe rupture is more often occult on presentation. The most frequent sites of rupture are not easily visualized, and more superficial injuries may block examination of the posterior segment. Very small sharp foreign bodies can enter the eye through small wounds that are difficult to visualize.
Our institution has developed the following protocol for evaluation of globe ruptures which are clinically apparent.
- Examine patient and confirm open globe injury based on clinical findings.
- Take digital photograph of open globe injury. Ideally the digital photograph will be placed into patient’s electronic medical record.
- Place plastic eye shield to protect open globe injury. No further examination of eye will occur.
- Consult Ophthalmology and communicate that a patient with an open globe is in the ED.
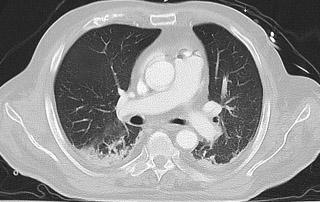
- Perform CT scan of head or if possible, selective CT of orbits, to rule out for retained foreign body. Plastic eye shield will remain over eye during CT scan.
- Give IV antibiotics in Emergency Department (Ciprofloxacin, Gentamicin and Vancomycin).
- Expedited patient to OR for exploration and primary closure of open globe.
[…] discussed in a previous post our algorithm for evaluation of clinically apparent globe injuries. However, this is less frequent than evaluating a patient with no clinically obvious globe […]