The patient is 79-year-old women has severe aortic stenosis and 2-vessel coronary artery disease s/p coronary artery bypass graft who lives independently and is very active who presented to the emergency department for acute dyspnea.
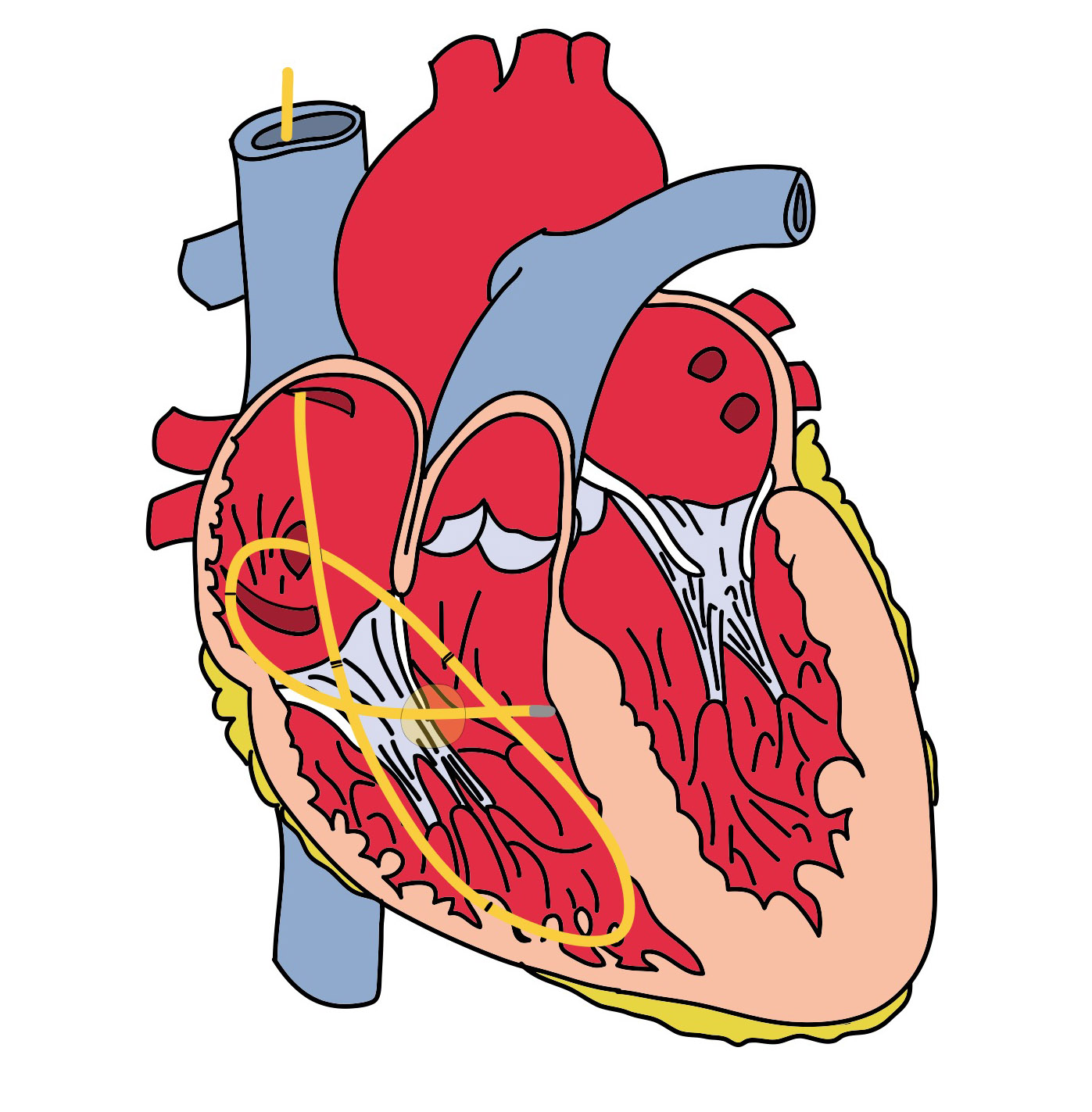
Seven years earlier she was diagnosed with coronary artery disease. Cardiac catheterization at the time showed a left dominant system with moderate stenosis of the proximal LCx and severe stenosis of proximal PDA, and severe stenosis of the proximal LAD. She had a saphenous vein skip graft to the LCx and PDA, and a internal thoracic artery (LIMA) graft to the mid-LAD. She has declined surgery for her aortic stenosis and has a valve area of 1.1 cm2. Her coronary artery anatomy is shown in the figure below.
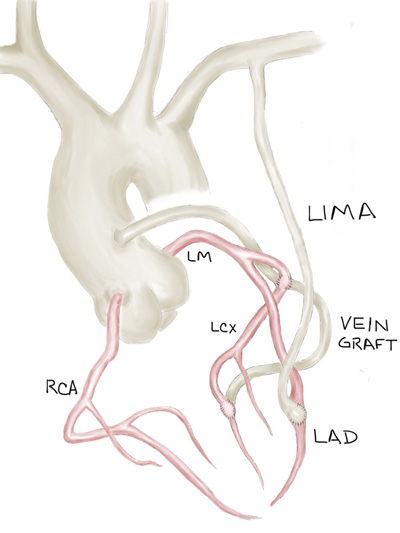
Native coronary arteries and a vein skip graft to proximal LCx then PDA and LIMA to mid-LAD.
On the day of presentation, she had been doing several loads of laundry, going up-and-down the stairs to her basement about six times. On her last trip she had developed severe shortness of breath. She did not experiencing any chest pain. She was so dyspneic however, that she called her daughter to have her bring her to hospital to “be looked at”. Her daughter was able to arrive with 5 minutes, but the patient was so short of breath she couldn’t walk. EMS was notified who brought the patient to the emergency department.
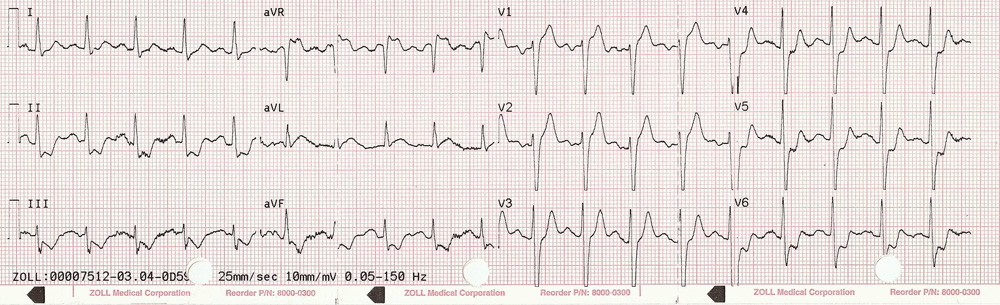
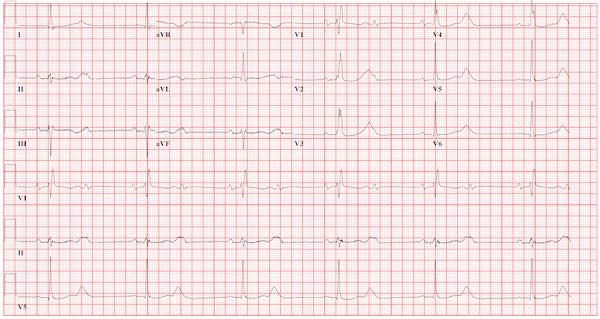
Prehospital ECG with 2mm of ST-segment elevation in V1, V2, V3, and aVR with diffuse ST depression.
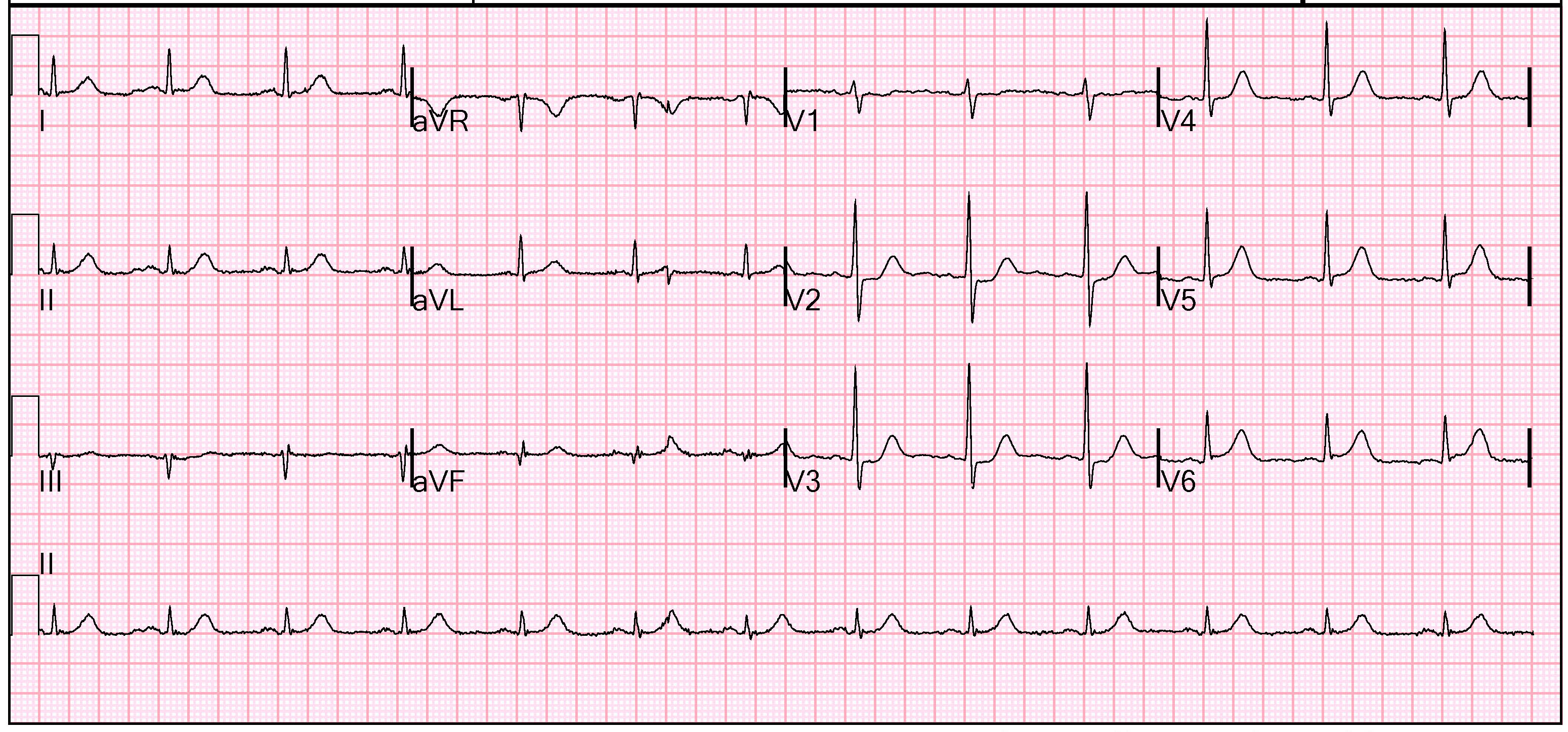
During transport, a 12-lead ECG was obtained. There is 2mm of ST-segment elevation in V1, V2, and aVR, with diffuse ST-depression through the remainder of the leads. On arrival in the emergency department she underwent an expedited an expedited evaluation. She was treated with an aspirin. Her vital signs were normal except for tachypnea. A 12-lead ECG was obtained, which was similar to the one obtained prehospital.
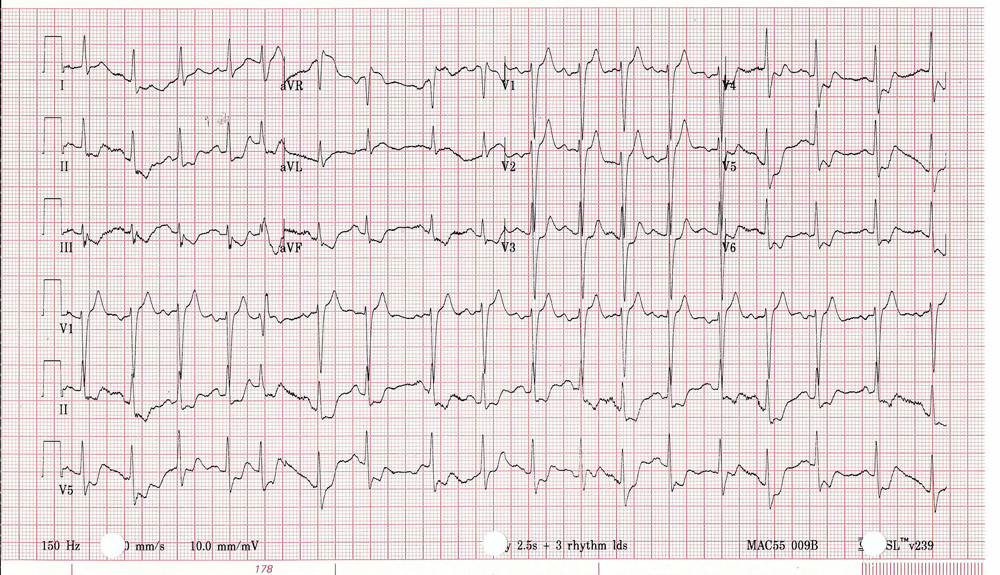
Presenting 12-lead ECG
She was taken to the cardiac catheterization lab for emergent angiography and possible PCI. Unfortunately there were substantial problems. The vein graft was chronically occluded which had been the blood supply to the LCx and PDA. There was a large subclavian artery acute plaque rupture proximal LIMA cutting off its blood supply. It had been the main blood to the LAD and anterior heart, and by collaterals the lateral and posterior heart. Fortunately, there were well developed right to left collaterals. Multiple attempts to reperfuse the subclavian artery were unsuccessful.
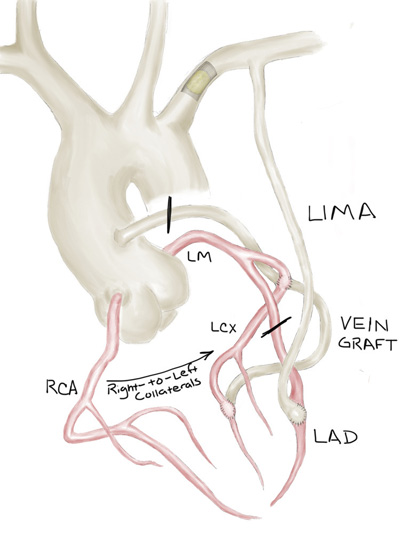
Coronary artery anatomy with subclavian plaque rupture and stenoses.
The elevation in V1 and V2 were seen in previous ECGs. These changes were attributed to LV aneurysm for old ischemic damage prior to her original bypass surgery.
Her peak troponin I was 65 ng/mL. Unfortunately, the patient developed profound cardiogenic shock. She had clear advance directives so further aggressive interventions were not pursued. The patient was transitioned to comfort cares.
This is a very interesting and unusual case of acute subclavian thrombosis causing acute coronary syndrome. I had not seen this before. The thrombosis usually arises secondary to damage to the intima of the artery in the setting of atherosclerotic disease. This damage can occur as a result of external muscular compression and repetitive stress to the artery, atherosclerotic changes to the vessel, or inflammatory processes.
References
- Ann Thorac Surg 2009 Dec;88(6):2036. Subclavian artery thrombosis associated with acute ST-segment elevation myocardial infarction.
- Ann Surg 1963 January;157(1):48. Subclavian Arterial Occlusion.
Contribute your thoughts.