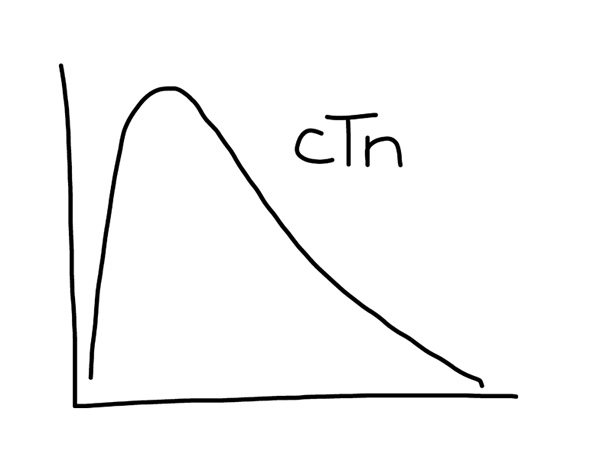
Our assay sensitivity for troponin has significantly increased, which lowers its specificity. While measurement of troponin levels are a very routine test in acute presentations, a good differential beyond acute coronary syndrome is necessary.
- Cardiac contusion
- Ablation, pacing.
- Congestive heart failure (acute or chronic).
- Aortic dissection
- Aortic valve disease
- Hypertrophic cardiomyopathy
- Tachyarrythmias, bradyarryhtmias, or heart block
- Apical ballooning syndrome
- Rhabdomyolysis with cardiac injury
- Pulmonary embolism
- Severe pulmonary hypertension
- Renal Failure
- Acute neurological disease (including stroke, SAH)
- Infiltrative disease (amyloidosis, hemochromatosis, sarcodoisis, or scleroderma0.
- Inflammatory diseases (myocarditis, pericarditis, myocardial extension of endocarditis)
- Drug toxicity or toxins
- Critically ill patients, especially with respiratory failure or sepsis
- Burns, especially if >30% TBSA
- Extreme exertion

Its important to understand that in the US the FDA has not yet approved the high-sensitivity (hs) troponin assays. Therefore we are still talking about the so-called contemporary troponin assays. The current assay is a good test, and the high-sensitivity troponin will have even better from an analytical perspective at lower values.
In either case the “differential” is not as important as WHEN to order it. With increased sensitivity (primarily when hs assays are here) there will be more positive values. Therefore adequate clinical judgement is primordial.
In other words, yes, cardiac contusion, burns, sepsis, etc can be part of the differential.
But the take-home point for all clinicians, especially the ones placing the first order (usually in ED), would be to
use the test wisely, weighing in pre-test probability and understanding the basics of the test such as coefficient of variation (CV) and the 99th percentile.
We do not usually order D-dimer in patients with sepsis or post-surgery for example. Why would you?
Same with troponin.
Order the test in patients with a suspicious for ischemia and working up for ACS.
Otherwise, you will deal with many positive values that might not change your plan, but even trigger potentially unnecessary work up and evaluation.
In conclusion, a test is as good as the physician who orders it.
[…] Dr. Yader Sandoval, made a very insightful comment about the use of tropnins on an earlier post (DDx Troponin Elevation). I felt it was so educational I wanted to highlight it. You can follow Dr. Sandoval on twitter […]
[…] debate was was raised by the fact that we recently switched assays as raised in a previous post. I must emphasize again, that there are NO hs-troponin available in the U.S. for clinical practice […]