Examples of failure modes include:
- Acute perforation
- Dislodgement
- Infection
- Vein thrombosis
- Migration
- Conduction failure
- Insulation damage/Externalization
Silicone Structural Failure
The last item, insulation failure has been seen in several lead designs. The silicone casing around transvenous leads is subjected to conditions that can lead to fracture and structural failure.
The proximal length undergoes high muscular stress from the pectoral muscles. Being above the bony thorax wall it is also subjective to crush, causing lead-to-lead or lead-to-can disruption. The distal segment experiences high intracardiac forces and dynamic flexing. There are also fatigue initiation points where the shocking coil is attached to the silicone. The most common site was the part of the lead just below the tricuspid valve.
The failure rate is higher in lead designs with dual shocking coils, which has contributed to recommendations against their use.
When the insulin fails, the defibrillation or sensing wires can be externalized. If their ETFE coating remains intact the externalized conductors remain electrically silent, and no detectable electrical abnormalities may be seen. However, the ETFE coating is not design to withstand the externalized environment. The coating often quickly becomes damaged, and leads to electrical short circuits.
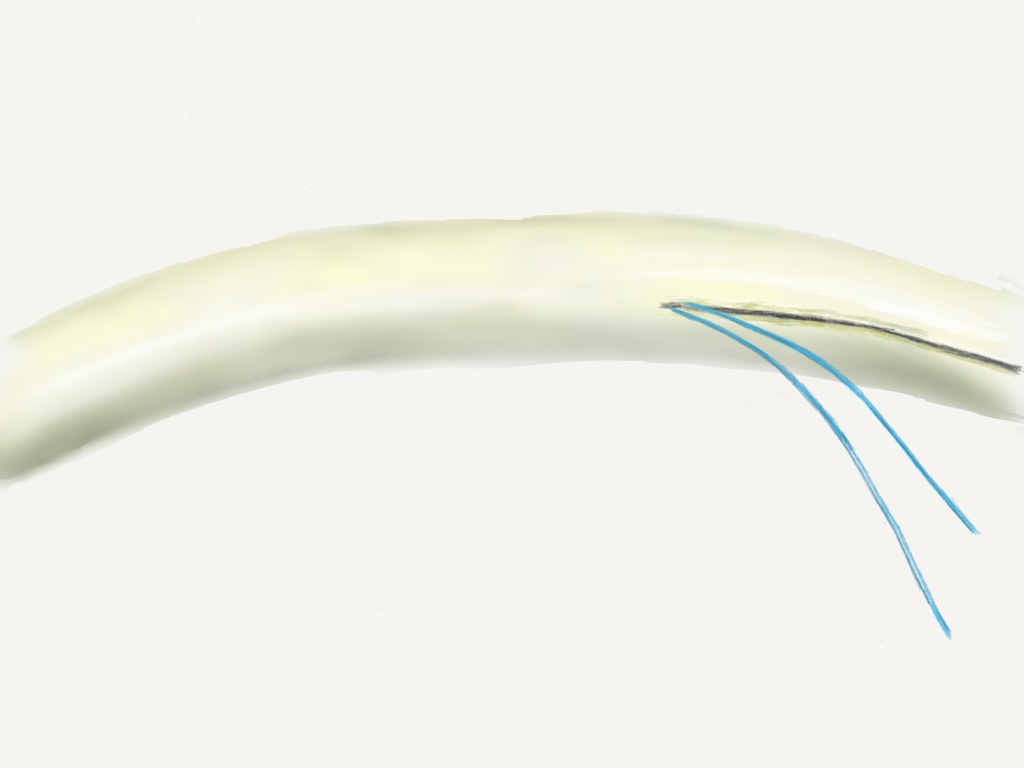
Structural failure of the pacemaker/ICD lead silicone casing and externalized conductors.
Asymmetric Lead Design
This problem was faced by St. Jude Medical with their Riata silicone-insulated leads, and led to a physician advisory. The cross section of a typical asymmetrical lead design (Riata family) is shown below.
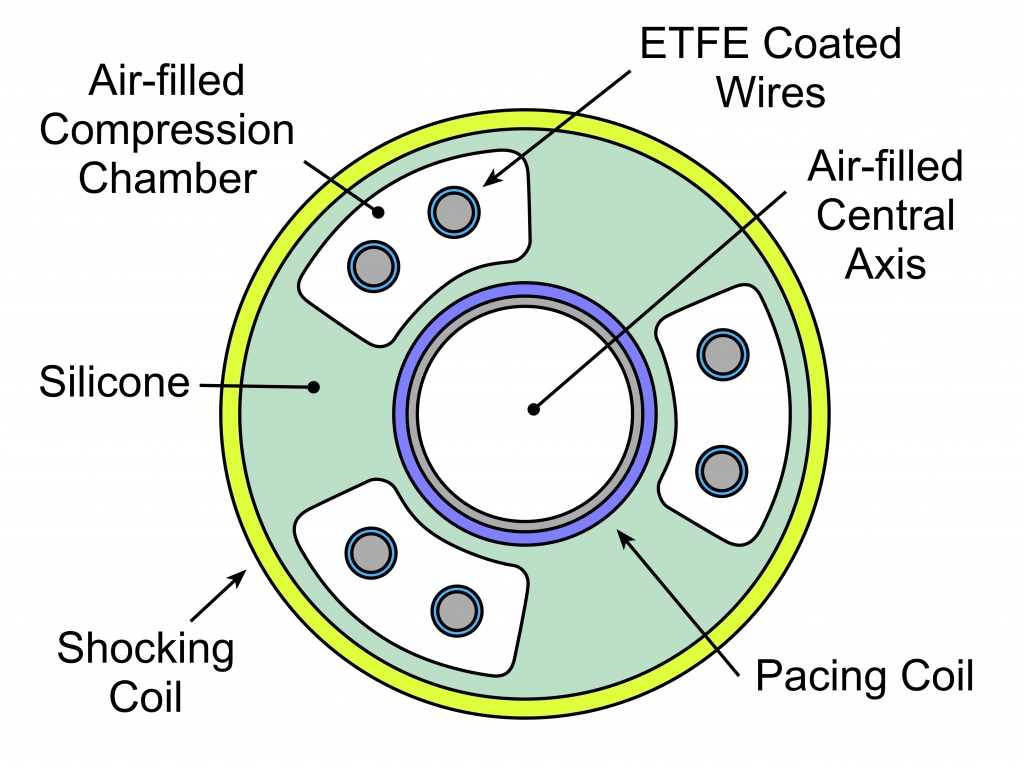
Schematic cross section of a pacemaker/ICD lead. Asymmetric design with redundant defibrillation and sensing wires.
A silicone casing forms the main component of the lead. The shocking coil rests on the outside of silicon. There are four chambers within the silicone. Redundant conductors carry the sensing and dual defibrillation wires, in three distributed compression chambers. A central axis chamber facilitates the use of a stylet during insertion, and is surrounded by the central pacing multifilar conductor.
Detecting Lead Structural Failure
Silicone structural failure events usually showed up 4-5 years after implantation and are diagnosed either in asymptomatic patients undergoing routine imaging, or more commonly after changes in electrical conduction are discovered with interrogation of malfunctioning devices.
Fluoroscopy has demonstrated to have positive and negative predictive values of 88% and 99%, respectively, and is the gold standard method. Small studies have suggested to chest radiography may be adequate screening tool, but this has not been widely adopted.
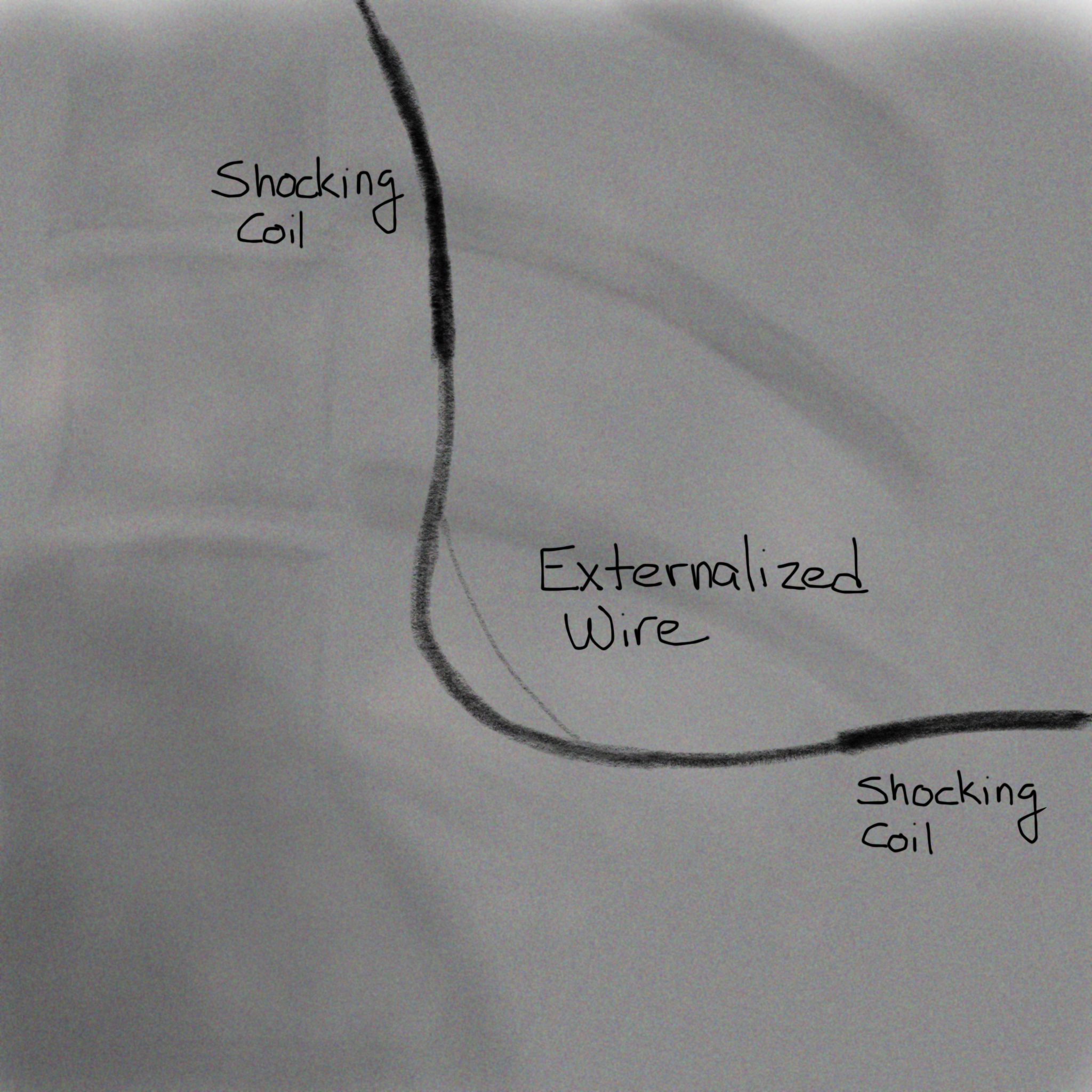
Fluoroscopy image of failed Pacemaker ICD Lead with externalized wire
Echocardiography can not reliably visualize a structurally failed lead or externalized conductors, but should be able to demonstrate any intracardiac thrombus that has formed.
Complications of Structural Lead Failure
Besides electrical failure, the externalized conductors are highly thrombogenic and can causes thrombus formation. This can usually be treated with systemic anticoagulation, though the extent of the clot and secondary effects such as SVC Syndrome may require explanation of the leads.
Unfortunately, for patients that have had these leads implanted, there are no recommendations for screening intervals or long-term follow up. Routine removal of the leads is not recommended. In the setting of thrombus formation, systemic anticoagulation should be pursued before either surgical or transvenous removal of the leads.