Sometimes imaging can reveal remarkable physiology.
A 40-year-old man presented with profound fatigue and abdominal pain that had begun the day before but substantially worsened over the last 12 hours. He reported not experiencing any chest pain, shortness of breath, nausea/vomiting. He was hypotensive, systolic blood pressure in 90s mmHg, and tachycardia at 105-110 bpm. He appeared premorbid on initial assessment.
Electrocardiogram was bland with only non-specific ST-segment and T-wave changes. Laboratory evaluation revealed a large lactic acidosis of 10 mmol/L. He was given 1000 mL of 0.9% saline. Despite unexplained shock, no bedside ultrasonographic evaluation was performed at this time.
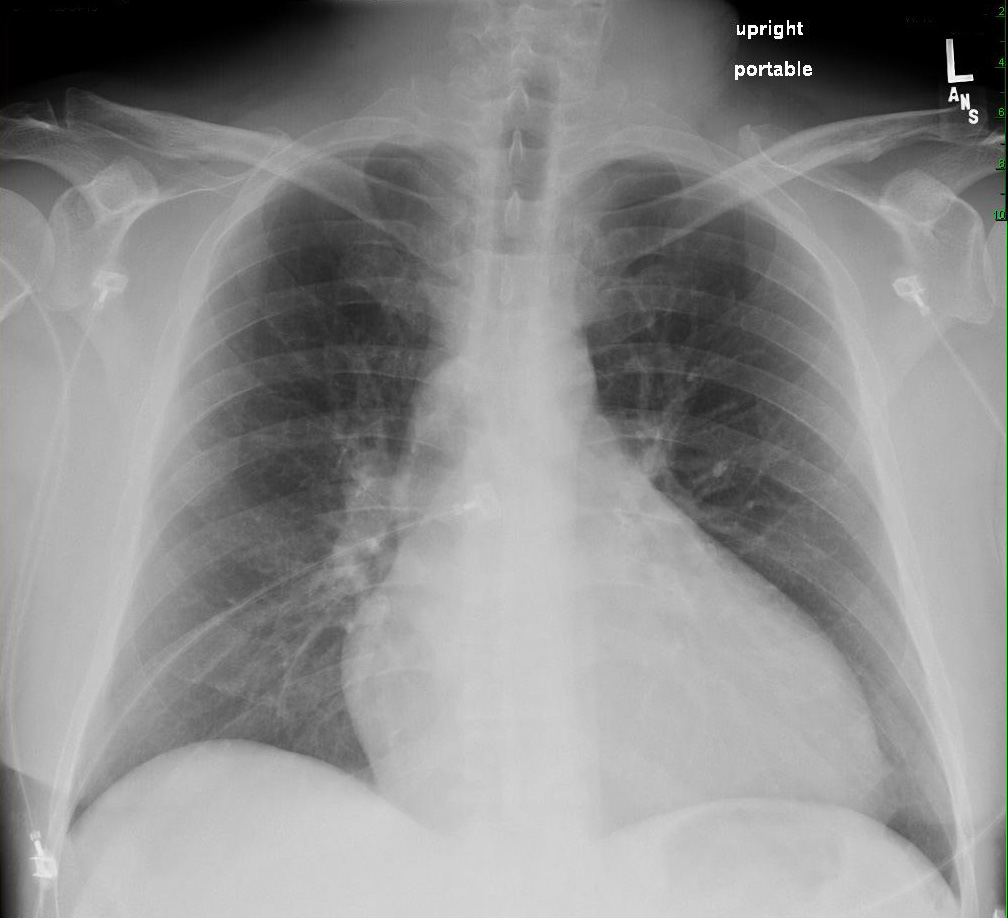
A chest radiograph was obtained (shown below), which shows cardiomegaly, but non-congestive lung fields.
Given the abdominal pain, a CT abdomen/pelvis was obtained with oral contrast material and 75 mL of Optiray-300 IV.
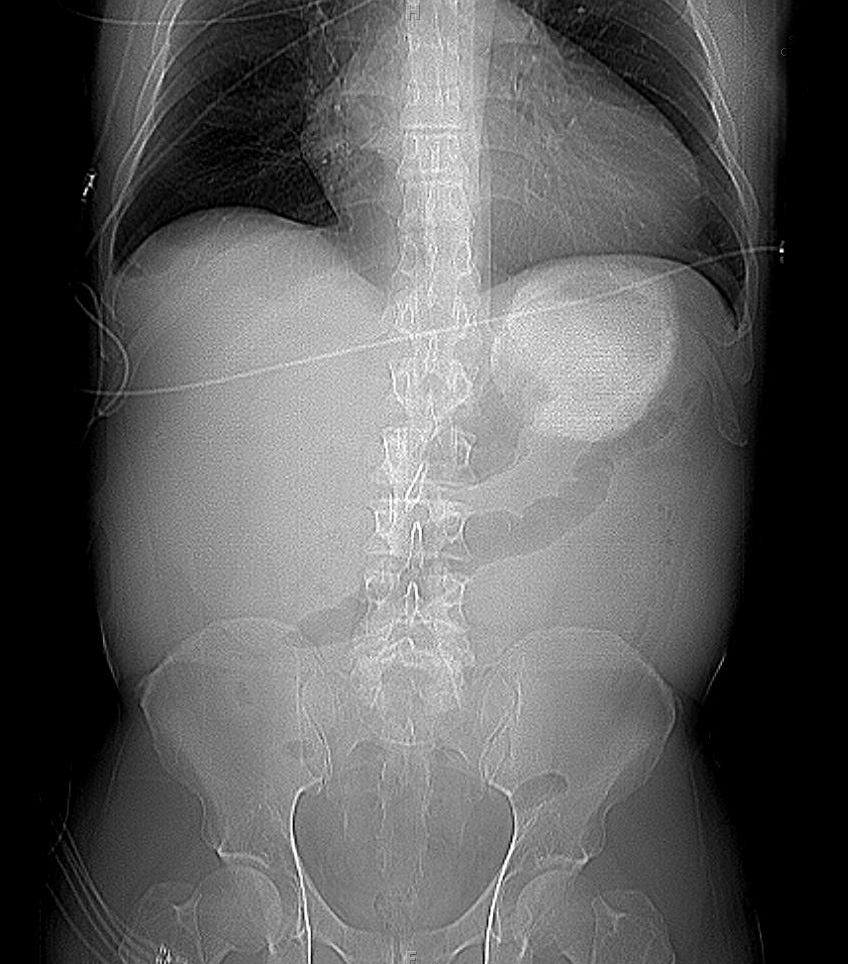
The scout film shows the oral contrast bolus in the stomach, and a paucity of bowel gas.
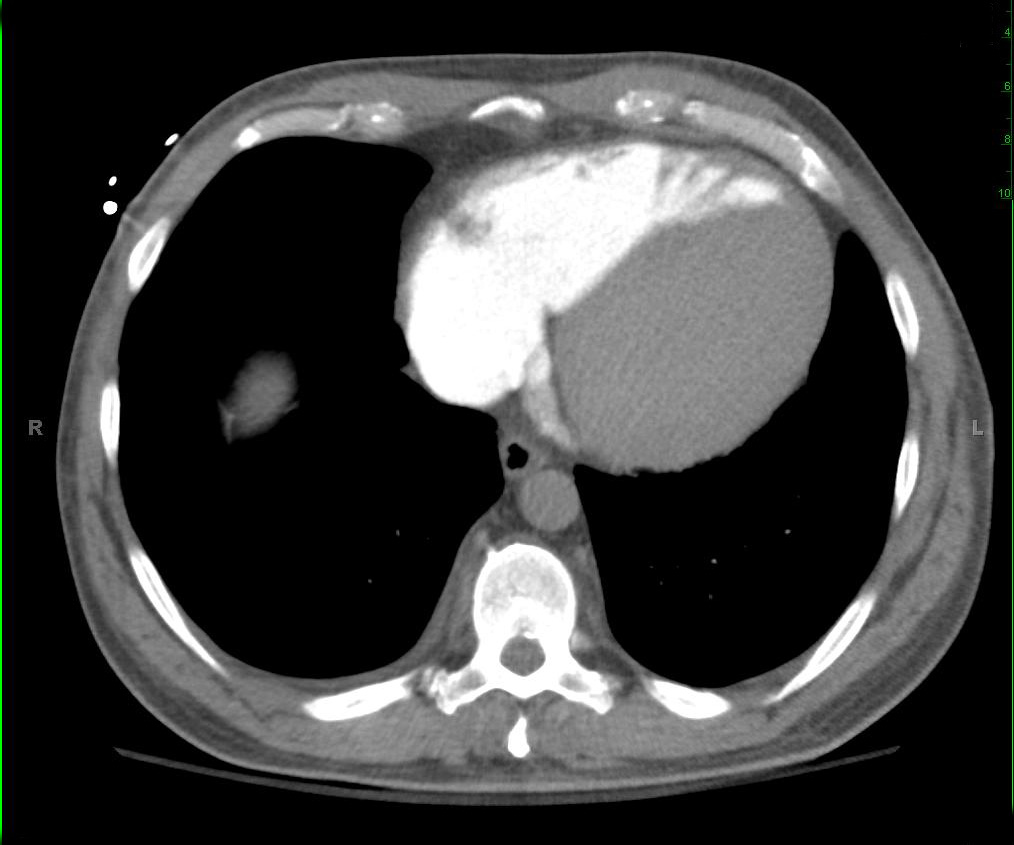
The coronal view, however, gives us the first hint of the underlying pathology. There is intravenous contrast material in the inferior vena cava and hepatic veins. The oral contrast bolus can be clearly seen in the stomach.

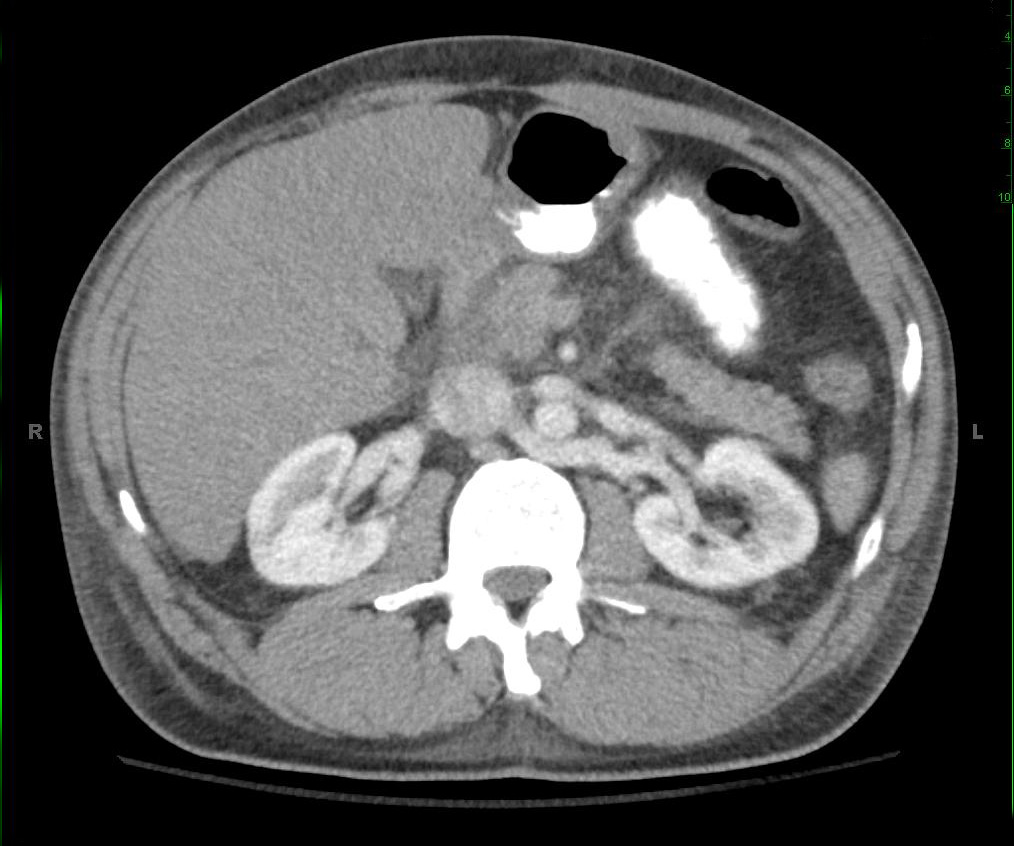
Cross sectional images at the level of the heart and kidney show there is almost complete lack of arterial contrast and the the venous contrast descending to the infrarenal IVC.

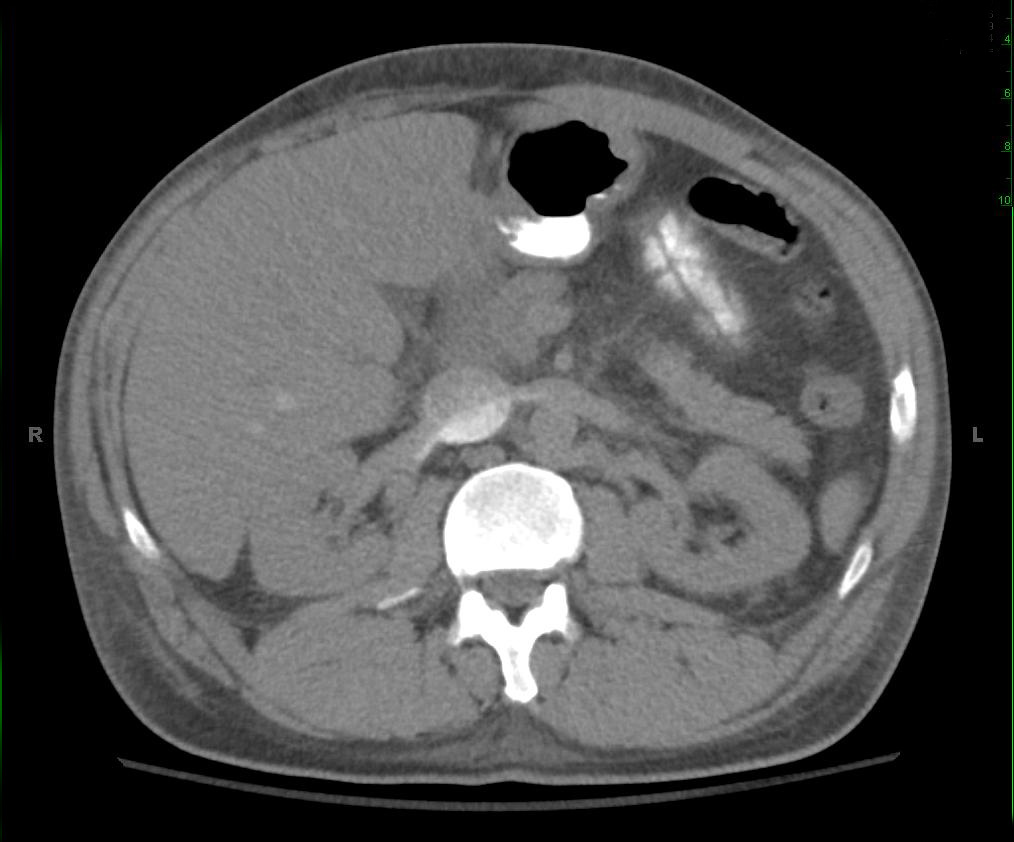
There is a considerable delay in arterial opacification of abdominal and pelvic organs. On additional delayed images, nephrogram persists in both kidneys. Overall findings suggest hypotensive state.
2-minute delay image at same cross-section level.
5-minute delay image at same cross-section level.

The finding of retrograde opacification of the IVC and hepatic veins during IV contrast studies has been associated with right-sided heart disease such as tricuspid regurgitation, pulmonary hypertension, and right ventricular systolic dysfunction. This sensitivity of this finding is increased with slower injection rates.
However, in this patient the lack of antegrade contrast motion represented profound cardiogenic shock. A bedside echocardiogram at this point showed profound hypodynamic contractility and no pericardial effusion. The patient was started on aggressive inotropic support, and taken emergently to the cardiac catheterization laboratory. Ventriculography demonstrated an ejection fracture <5% and diffuse coronary spasm. Unfortunately, he developed electromechanical dissociation, and was unable to be resuscitated. His presenting abdominal pain was attributed to ischemic gut from hypoperfusion.
References
1. Am J Roent 2004;183:1227.

Contribute your thoughts.